
Lipoid Pneumonia
Authors:
Jonathan Popler, MD
Georgia Pediatric Pulmonology Associates, Atlanta, Georgia
Ann Beach, MD
Scottish Rite Pediatric and Adolescent Consultants, Children’s Healthcare of Atlanta, Georgia
Citation:
Popler J, Beach A. Lipoid pneumonia. Consultant for Pediatricians. 2015;14(7):334.
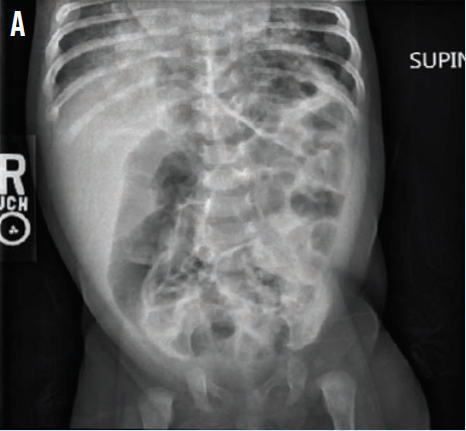
A 7-week-old girl presented with a chief concern of fussiness. The physical examination revealed a well-appearing infant. Abdominal radiographs showed a nonspecific bowel gas pattern, along with an incidental finding of opacities in both lower lungs (A).
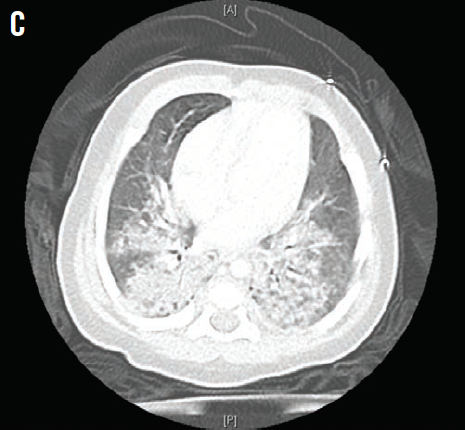
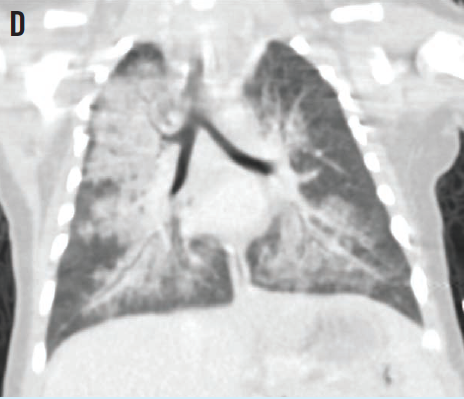
Chest radiographs and a follow-up chest computed tomography scan revealed patchy, bilateral alveolar infiltrates. The infant’s lungs demonstrated abnormal multifocal airspace opacifications of the right upper lobe, the right middle lobe, and the medial lower lobes bilaterally, in subsegmental distribution (B). Patchy alveolar infiltrates were visible diffusely throughout both lungs, with relative sparing of the left upper and right middle lobes (C and D).

A more extensive history revealed that the parents had been feeding the infant 15 to 30 mL of olive oil daily for constipation. Based on the history and clinical and radiographic findings, the patient received a diagnosis of lipoid pneumonia secondary to aspiration of olive oil.
Making the unusual diagnosis of lipoid pneumonia secondary to aspiration of oil can be difficult, because symptoms, signs, and radiographic findings are nonspecific. Aspiration may not be obvious, because oil may not trigger a cough reflex.
The differential diagnosis of diffuse infiltrates on chest imaging of a neonate includes bronchopulmonary dysplasia, neonatal lung disease (eg, interstitial lung disease), aspiration syndromes, and congenital heart defects.