
Peer Reviewed
Early Recognition and Management of Lithium Battery Ingestion in a 15-Month-Old
A 15-month-old boy was brought to an urgent care center by his father for suspected ingestion of a button battery.
History. The father noticed a remote control lying on the floor where his toddler was playing; the back had been removed and the newly placed lithium battery was missing. He was asymptomatic, including no unusual fussiness, drooling, wheezing, vomiting, or cyanosis.
His vital signs were within normal limits. A thorough physical examination revealed moist mucous membranes, no oral lesions or ulcerations, a soft and non-tender abdomen, bowel sounds within normal limits, and no significant abnormalities. The patient was born full term without complications. He was otherwise healthy.
Diagnostic testing. Nose-to-rectum plain X-rays were taken immediately upon arrival. The X-ray results confirmed a solitary opaque circular object in the distal stomach (Figure 1).

Figure 1. Anteroposterior view of nose-to-rectum plain radiograph revealing an opaque, coin-shaped mass suspected to represent ingested button battery based on patient’s history.
Differential diagnoses. It is crucial to accurately differentiate between a button battery and a coin when examining plain radiography, as prompt removal of button batteries via endoscopy is necessary whereas the urgency of removing coin(s) may vary depending on the circumstances. When analyzing an anterior-posterior X-ray for any round, opaque foreign object, close inspection is recommended to identify a double ring or halo sign, indicative of a button battery, as opposed to the completely homogenous radiopacity of an ingested coin.1 Additionally, obtaining a lateral plain film radiography may aid in detection, as some batteries may display a step-off sign.1 However, thinner battery designs may resemble a coin on lateral images alone.1 Upon closer examination of Figure 1, the patient’s anterior-posterior radiograph image reveals an opaque circular foreign object with a double ring, confirming the presence of a button battery in the gastric antrum in conjunction with the patient’s parental history.
Treatment and management. Based on the initial concern of potential battery ingestion, the patient received 10 mL of oral honey during triage and was promptly sent for imaging. Upon confirmation of the battery and its location on imaging, the child was transferred via ambulance to a children’s hospital equipped to perform emergent foreign body removal via esophagogastroduodenoscopy (EGD). EGD exploration revealed no gross damage of the esophagus. Mild gastric ulcerations with surrounding inflammation were noted and neutralized with acetic acid (Figure 2). A 20 mm lithium battery was successfully retrieved from the prepyloric region, approximately 3 to 4 hours after suspected ingestion (Figure 3).
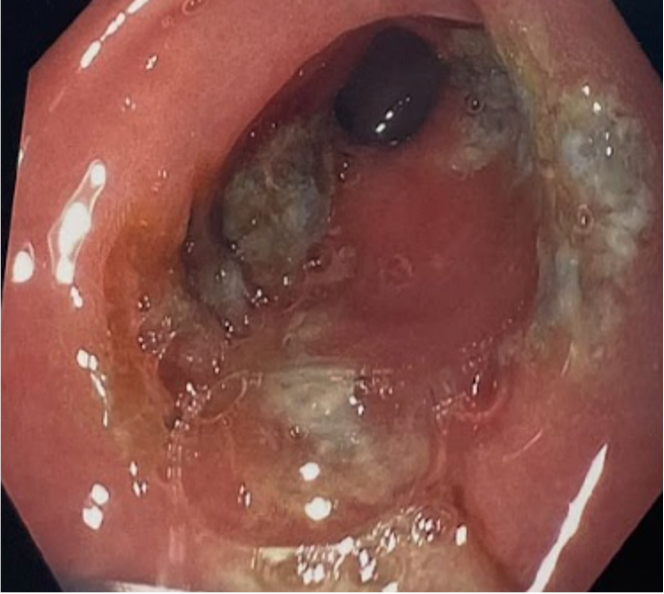
Figure 2. Superficial erosions noted in the distal stomach on EGD imaging post-neutralization with acetic acid.

Figure 3. Previously new 20 mm lithium battery after endoscopic retrieval, showing signs of erosion 3 to 4 hours post-ingestion.
Outcome and follow-up. The patient received a dose of intravenous pantoprazole and was subsequently discharged the same day. The patient was prescribed oral omeprazole 10 mg daily for 1 month. The patient experienced a speedy recovery without complications.
Discussion. The age of advancing technology and the widespread use of battery-powered household devices have contributed to a rising trend in accidental pediatric battery ingestions, particularly of lithium coin batteries due to their conveniently small size.2 Battery-related incidents in children under 18 years old surged from 2010 to 2019 with over 7000 annual emergency visits, which is double from the previous decade.3 Foreign body ingestions are overall more common in children aged younger than 3 years old due to the explorative nature and oral fixation associated with this age group.4,5 A majority of patients are asymptomatic after initial ingestion of a battery which may contribute to a delay in diagnosis and a higher complication rate, especially in unwitnessed cases.4,5 Maintaining a high level of suspicion and initiating prompt workup and treatment is crucial in avoiding serious injury and potential death.2,6,7
The active portion of a battery consists of a negative terminal (commonly made of zinc or lithium) and a positive terminal (commonly made of lithium manganese, manganese dioxide, oxygen, silver oxide, or mercuric oxide).8,9 When a battery is in contact with bodily tissue its electrical potential triggers an isothermic water hydrolysis reaction at the battery’s negative pole junction.9 This results in the production of hydroxide ions due to the electrical current flowing through adjacent tissue, effectively “completing the circuit” between the two poles of the button battery.9 The rapid accumulation of hydroxide ions can elevate local tissue pH to alkaline levels as high as a pH of 12 to 13, which may subsequently induce liquefactive necrosis and deep caustic injury.9 The severity of tissue damage after button battery ingestion depends upon the remaining amount of electrical charge in the battery, the length of time the battery is in the upper gastrointestinal tract, and the battery size.9-11 However, the ingestion of a “dead” or inactive button battery is still of major concern because it can retain enough voltage to generate an external current.12
Epithelial damage is evident as soon as 15 minutes after impaction and major corrosive injury can occur in as little as 2 hours.6,8 The esophagus is the most prone anatomical location for ingested battery impaction and tissue damage.11,13 Esophageal tissue becomes edematous and the battery adheres tightly to the mucosa the longer the battery is impacted.11 Tissue necrosis leads to erosion, which can result in esophageal perforation over days to weeks, with the risk of eventual formation of fistulae between the esophagus and neighboring structures such as the trachea or aorta.6,13 Mucosal injury and subsequent complications increase with button batteries larger than 20 mm in diameter and in children under 5 years of age.6 Larger batteries are more difficult to pass through the narrow esophagus of a young child, resulting in more severe burns and tissue damage within a shorter period of time.10,13-15 Prolonged battery impaction in the esophagus may result in vocal cord paresis and paralysis, tracheal stenosis, esophageal perforation, esophageal stenosis, tracheoesophageal fistula (TEF), vascular fistula, and hemorrhage.7,16 Hemorrhage from vascular injuries, primarily aortoesophageal fistulas, is the most commonly reported cause of death in patients after button battery ingestion.11,17 Button batteries in the stomach are thought to be less damaging due to the larger cavity size, increased wall thickness, and less anatomic structures in the vicinity to endure potential collateral damage.18,19
Regardless of presenting symptoms or lack thereof, when button battery ingestion is suspected or known, an emergency evaluation including nose-to-rectum plain radiographs is recommended for all children 12 years of age and younger, all batteries 12 mm in diameter or greater, or if the battery size is unknown.7 Imaging may be deferred, however, for asymptomatic, healthy patients older than 12 years who have ingested a single battery less than 12 mm in size, no concomitant magnet ingestion, no existing history of esophageal abnormalities, and a reliable caregiver to observe for battery passage at home with instructions to seek prompt treatment if symptoms develop or if battery passage has not been confirmed after 7 to 14 days.7,20
Oral administration of 10 mL of pure honey, repeated every 10 minutes as necessary, is advised for children aged 1 year or older with known or suspected battery ingestion within 12 hours.14,20 An appropriate alternative for infants less than 1 year of age or children with a honey allergy is to administer 1 g of oral sucralfate every 10 minutes.20 In 2018, Anfang and colleagues conducted a study to explore the potential protective effects of various substances in cases of button battery ingestion, including apple and orange juice, sports drinks, honey, maple syrup, and sucralfate. Their initial ex vivo testing demonstrated that honey and sucralfate could neutralize the effects of the batteries. Subsequent testing in a porcine animal model confirmed the efficacy of these substances in vivo. To determine the optimal dosage and frequency, the authors administered 10 ml of each substance every 10-15 minutes, mimicking physiological saliva production. Similar studies in 2021 and 2022 also found that honey reduced tissue injury compared with other substances and saline used as a control.21,22 If an X-ray reveals a battery in the esophagus, honey can be continued up to 6 doses or sucralfate up to 3 doses.20 No further doses are needed for batteries located in the stomach or beyond.14,20
Per the 2021 guidelines for clinical management of button battery ingestion from the Children’s Healthcare of Atlanta, the timing of battery removal via direct endoscopic visualization depends on the size and/or location of the button battery.20 Emergent endoscopic removal within 2 hours is recommended for all esophageal impacted batteries, as well as for batteries in the stomach if symptomatic or co-ingested with a magnet.8,19,20 Endoscopic removal within 24 hours is recommended for batteries in the stomach if the patient is asymptomatic, 6 years of age or younger, the battery is 15 mm or greater, or with multiple battery ingestion.20 Gastroenterologist consultation without the need for endoscopic removal may be appropriate for previously healthy patients aged 7 years or older who are asymptomatic and have ingested a battery smaller than 15 mm that is located in the stomach or if the battery has passed the pylorus.20 These patients may be monitored in the outpatient setting and counseled to return for imaging or further management if the battery has not passed naturally within 7 to 14 days or if symptoms develop.20
Preventative measures for button battery ingestion includes counseling caretakers on the importance of properly storing batteries out of reach of children, as well as vigilantly monitoring toddlers and children at all times.5 President Biden’s recent enactment of Reese’s Law, which mandates child-resistant testing standards and prominent warning labels for button battery-powered devices (effective February 23, 2023), further serves to augment efforts to prevent incidences of accidental battery ingestions.23
Conclusion. This case serves to emphasize the unfortunate rise in battery-related incidents among children. Our patient was fortunately met with a favorable outcome, largely due to early recognition by the parent, prompt protocol initiation by the urgent care staff, and the culmination of well-orchestrated efforts of the emergency medical team and pediatric gastroenterology specialist. Patients from all ethnic and socioeconomic backgrounds are at risk for encountering the dangers of accidental foreign body ingestion, thus highlighting the importance of health care professionals to provide anticipatory guidance to all parents/guardians, and particularly those with young children.
References:
- Jatana KR, Litovitz T, Reilly JS, Koltai PJ, Rider G, Jacobs IN. Pediatric button battery injuries: 2013 task force update. Int J Pediatr Otorhinolaryngolo. 2013;77(9):1392–1399. doi:10.1016/j.ijporl.2013.06.006
- Speidel AJ, Wölfle L, Mayer B, Posovszky C. Increase in foreign body and harmful substance ingestion and associated complications in children: a retrospective study of 1199 cases from 2005 to 2017. BMC Pediatrics, 2020;20(1):1–10. doi:10.1186/s12887-020-02444-8
- Chandler MD, Ilyas K, Jatana KR, Smith GA, McKenzie LB, MacKay JM. Pediatric battery-related emergency department visits in the United States: 2010-2019. Pediatrics. 2022;150(3):e2022056709. doi:10.1542/peds.2022-056709
- Chan YL, Chang SS, Kao KL, et al. Button battery ingestion: an analysis of 25 cases. Chang Gung Med J. 2002;25(3):169–174. http://cgmj.cgu.edu.tw/2503/250304.pdf
- Isa HM, Aldoseri SA, Abduljabbar AS, Alsulaiti KA. Accidental ingestion of foreign bodies/harmful materials in children from Bahrain: a retrospective cohort study. World J Clin Pediatr. 2023;12(4):205-219. doi:10.5409/wjcp.v12.i4.205
- Akinkugbe O, James AL, Ostrow O, Everett T, Wolter NE, McKinnon NK. Vascular complications in children following button battery ingestions: a systematic review. Pediatrics. 2022;150(3):e2022057477. doi:10.1542/peds.2022-057477
- Semple T, Calder AD, Ramaswamy M, McHugh K. Button battery ingestion in children-a potentially catastrophic event of which all radiologists must be aware. Br J Radiol. 2018;91(1081):20160781. doi:10.1259/bjr.20160781
- Litovitz T, Whitaker N, Clark L, White NC, Marsolek M. Emerging battery-ingestion hazard: clinical implications. Pediatrics. 2010;125(6):1168–1177. doi:10.1542/peds.2009-3037
- Sethia R, Gibbs H, Jacobs IN, Reilly JS, Rhoades K, Jatana KR. Current management of button battery injuries. Laryngoscope Investig Otolaryngol. 2021;6(3):549–563. doi:10.1002/lio2.535
- Anfang RR, Jatana KR, Linn RL, Rhoades K, Fry J, Jacobs IN. pH-neutralizing esophageal irrigations as a novel mitigation strategy for button battery injury Laryngoscope. 2019;129(1):49–57. doi:10.1002/lary.27312
- Leinwand K, Brumbaugh DE, Kramer RE. Button battery ingestion in children: a paradigm for management of severe pediatric foreign body ingestions. Gastrointest Endosc Clin N Am. 2016;26(1):99–118. doi:10.1016/j.giec.2015.08.003
- Langkau JF, Noesges RA. Esophageal burns from battery ingestion. Am J Emerg Med. 1985;3(3):265. doi:10.1016/0735-6757(85)90111-1
- Maves MD, Carithers JS, Birck HG. Esophageal burns secondary to disc battery ingestion. Ann Otol Rhinol Laryngol. 1984;93(4 Pt 1):364–369. doi:10.1177/000348948409300416
- Lerner DG, Brumbaugh D, Lightdale JR, Jatana KR, Jacobs IN, Mamula P. Mitigating risks of swallowed button batteries: new strategies before and after removal. J Pediatr Gastroenterol Nutr. 2020;70(5):542–546. doi:10.1097/MPG.0000000000002649
- Orsagh-Yentis D, McAdams RJ, Roberts KJ, McKenzie LB. Foreign-body ingestions of young children treated in US emergency departments: 1995-2015. Pediatrics. 2019;143(5):1–8. doi:10.1542/peds.2018-1988
- Russell RT, Cohen M, Billmire, DF. Tracheoesophageal fistula following button battery ingestion: successful non-operative management. J Pediatr S. 2013;48(2):441–444. doi:10.1016/j.jpedsurg.2012.11.040
- Brumbaugh D, Colson SB, Sandoval JA, et al. Management of button battery-induced hemorrhage in children. J Pediatr gastroenterol Nutr. 2011;52(5):585–589. doi:10.1097/MPG.0b013e3181f98916
- Rebhandl W, Steffan I, Schramel P, et al. Release of toxic metals from button batteries retained in the stomach: an in vitro study. J Pediatr S. 2002;37(1):87–92. doi:10.1053/jpsu.2002.29435
- Khalaf RT, Ruan W, Orkin S, et al. Gastric injury secondary to button battery ingestions: a retrospective multicenter review. Gastrointest Endosc. 2020;92(2):276–283. doi:10.1016/j.gie.2020.04.037
- Button battery ingestion: clinical practice guideline. Children's Healthcare of Atlanta. Accessed September 25, 2023. https://www.choa.org/-/media/Files/Childrens/medical-professionals/clinical-practice-guidelines/button-battery-ingestion
- Gyawali BR, Guragain R, Gyawali DR. Role of honey and acetic acid in mitigating the effects of button battery in esophageal mucosa: a cadaveric animal model experimental study. Indian J Otolaryngol Head Neck Surg. 2022;74(3):5759-5765. doi:10.1007/s12070-021-02382-6
- Jia W, Xu G, Xie J, et al. Electric insulating irrigations mitigates esophageal injury caused by button battery ingestion. Front Pediatri. 2022;10. doi:10.3389/fped.2022.804669
- Consumer Product Safety Commission. Safety standard and notification requirements for button cell or coin batteries and consumer products containing such batteries, vol. 88, no. 27. Govinfo. Accessed September 10, 2023. https://www.govinfo.gov/app/details/FR-2023-02-09/2023-02356
AFFILIATIONS:
1Medical Student, Philadelphia College of Osteopathic Medicine, Suwanee, GA
2Assistant Professor of Family Medicine, Department of Family Medicine, Philadelphia College of Osteopathic Medicine, Suwanee, GA
CITATION:
Yoon A, Seo Y, Zarandy J. Early recognition and management of lithium battery ingestion in a 15-month-old. Consultant. 2024;64(3):e2. doi:10.25270/con.2024.03.000003.
Received October 17, 2023. Accepted February 2, 2024. Published online March 27, 2024.
DISCLOSURES:
The authors report no relevant financial relationships.
ACKNOWLEDGEMENTS:
None.
CORRESPONDENCE:
Joy Zarandy, DO, Philadelphia College of Osteopathic Medicine (PCOM) – Georgia Campus, 625 Old Peachtree Road NW, Suwanee, GA 30024 (joyza@pcom.edu)