
Pearls of Wisdom: Smoking Around Children
Tiffany is a 2-year-old with recurrent acute otitis media (AOM). She is in to see you again today with AOM—her fourth episode in the last 12 months. When asked, the parents said they both smoke, but not inside in the house.
For parents who say they don’t smoke in the house, is it good enough to minimize exposure for their children?
A. Yes. Smoking outside, if consistent, places the child at the same risk of nicotine exposure as a non-smoking home.
B. Yes. Smoking outside, if consistent, increases nicotine exposure, but only minimally, compared to a non-smoking home.
C. No. Smoking outside, if consistent, increases nicotine exposure about 25% more compared to a non-smoking home.
D. No. Smoking outside, if consistent, still produces nicotine metabolites at levels 5 times higher than a non-smoking home.
What is the correct answer?
(Answer and discussion on next page)
Louis Kuritzky, MD, has been involved in medical education since the 1970s. Drawing upon years of clinical experience, he has crafted each year for almost 3 decades a collection of items that are often underappreciated by clinicians, yet important for patients. His “Pearls of Wisdom” as we like to call them, have been shared with primary care physicians annually in an educational presentation entitled 5TIWIKLY (“5 Things I Wish I Knew Last Year”…. or the grammatically correct, “5 Things I Wish I’d Known Last Year”).
Now, for the first time, Dr Kuritzky is sharing with the Consultant360 audience. Sign up today to receive new advice each week.
Answer: Even amongst parents who say they only smoke outside, cotinine levels were still more than 5 times as high in children from these homes as non-smoking homes.
Acute otitis media can disrupt the life of a child as well as other family members. Merely attending to the management of the otitis does not take into account the impact of all the risk factors the child is exposed to—and that information is important in deciding whether or not to provide antibiotics, and even which antibiotics to prescribe, on the visit.
The clinician was wise enough to enquire about smoking. A sensible way to ask, to include the most possibilities, is to ask something akin to: “Does anyone in the child’s home or caretaking environment smoke?”
Note: You are not asking whether they smoke in the house, out of the house, around the child, not around the child, etc. It may be that Grandma smokes when the child is over at her house for the weekend or maybe a babysitter smokes. The bottom line is that we want to know if anyone who comes into consistent contact with the child is a smoker.
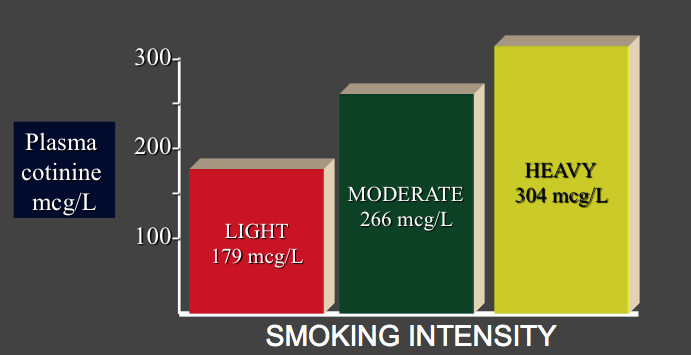
Table 1. Plasma Cotinine Reflects Smoking Intensity1
Many well-intended parents will happily respond saying, “Well, both of us smoke, but we don’t smoke in the house.” Is that good enough?
Clinical trials looking at a metabolite of nicotine, called cotinine, confirm that smoking outside is not good enough. Cotinine is useful as it is a long-term marker of cigarette smoking1 and, much like the A1c of diabetes, gives us a picture of long-term glucose levels. In addition, cotinine is readily measureable in children—in their saliva, urine, and blood—making access to fluid samples non-traumatic to children.
Table 2. Urinary Cotinine in Children Effect of At-Home Smoke2
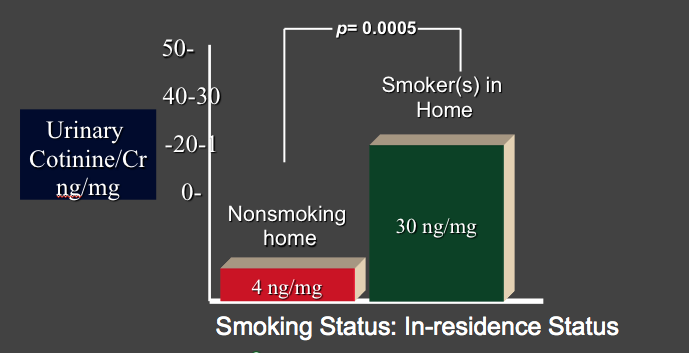
Because as many as 20% of American adults continue to smoke, most of us non-smokers still have measurable cotinine levels in our plasma. Winkelstein, et al2 compared urinary cotinine levels in children from non-smoking homes to homes with smokers. Table 2 indicates that cotinine levels were more than 7 times higher in children who lived in smoking homes than non-smoking homes—30 ng/mg Cr versus 4 ng/mg Cr.
Table 3. Don’t Worry Doc, We Only Smoke Outside!2
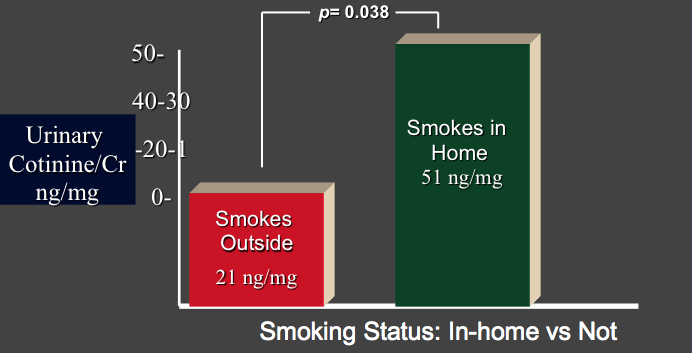
The next step of the investigation looked at a comparison within smoking homes of parents who said they only smoked outside versus those who did not attempt to prevent secondary smoke consequences. As shown in Table 3, even amongst parents who say they only smoke outside, cotinine levels levels were still more than 5 times as high (21 ng/mg) in children from these homes as non-smoking homes (4 ng/mg Cr).
Understanding Smoke Transmission
How is this smoke transmission occurring, if it is going on outside? Probably not a clinician amongst us has avoided the situation where a well ensconced smoker is seen in our office and we cannot comfortably invite other patients into that room for a protracted period of time despite air fresheners due to the residue of smoke and tobacco simply attached to the patient’s clothing, skin, and hair. Some of the parents are probably not being totally honest—there are probably times when little Tiffany is far away in another part of the house, or it’s raining or really cold outside, or “just this once”…the list of rationalizations for not being fully compliant with restricting smoking to outside the home is lengthy.
I commonly show parents and caregivers these very graphs (Table 1-3). I praise them for thinking of the well-being of their little one, but explain that smoking outside—though a step in the right direction—is not enough. If they really want to maximize risk reduction for their child, they must stop.
Some clinicians feel that approaching parents with this type of information is a “guilt trip.” Out of respect, I always mention that perspective in discussions with colleagues about smoking exposure and cotinine as I would certainly not want to be encouraging any clinician to go beyond his/her particular ethical boundaries. While I have found that sometimes this is perceived as a “guilt trip” by the parents or caregivers, over many years of practice I have yet to have a parent respond to this information with hostility or resentment.
Environmental tobacco smoke is a significant toxin, leading to increased risk for otitis, bronchitis, pneumonia, cough, wheeze, and asthma.3 When asthma occurs in children of smokers, they have more frequent and more severe exacerbations.3
Worldwide, lung cancer is the top cause of cancer death. Data emerging from Asia—as many as half of adult men smoke in China—indicate that the epidemic of lung cancer deaths we are currently experiencing shows little likelihood of abating, at least on a global basis. The United States has taken positive steps to eliminate smoking from restaurants, hotels, convention centers, and many other public places. The population at-risk from environmental exposure—children—deserves our further attention.
What’s the “Take Home?”
Environmental exposure of children to tobacco smoke is consequential. Laboratory studies confirm that the well-intended step of smoking outside is not sufficient. We should be taking environmental smoking histories in reference to our pediatric patients, and supplying appropriate advice, counseling, and pharmacotherapy to assist in smoking cessation.
- Lawson GM, Hurt RD, Dale LC, et al. Application of serum nicotine and plasma cotinine concentrations to assessment of nicotine replacement. J Clin Pharmacol. 1998;38:502-509.
- Winkelstein ML, Tarzian A, Wood RA. Parental smoking behavior and passive smoke exposure in children with asthma. Ann Allergy Asthma Immunol. 1997;78(4):419-423
- Kuehn BM. Tobacco smoke exposure among children. JAMA. 2013;310(12):1218-1219.