
Peer Reviewed
Acute Small Bowel Obstruction in Marfan Syndrome Unmasking a Rare Association
AUTHORS:
Suhas Ganguli, MD, DCH
Department of Pediatrics, Cohen Children’s Medical Center of New York, New Hyde Park, New York
Jennifer Nguyen Simpson, MD
Department of Pediatrics, Flushing Hospital Medical Center, New York, New York
Sonia Patel, MD
Department of Emergency Medicine, Flushing Hospital Medical Center, New York, New York
Susana Rapaport, MD
Department of Pediatrics, Flushing Hospital Medical Center, New York, New York
Partha Chatterjee, MD
Department of Pediatrics, Jamaica Hospital Medical Center, New York, New York
CITATION:
Ganguli S, Simpson JN, Patel S, Rapaport S, Chatterjee P. Acute small bowel obstruction in Marfan syndrome unmasking a rare association [published online October 2, 2017]. Consultant360.
A 15-year-old girl with Marfan syndrome presented with acute-onset epigastric pain and 20 episodes of nonbilious, nonbloody, nonprojectile vomiting over 10 hours. Her family history was significant for Marfan syndrome in her 2 siblings and her father.
Physical examination. Her vital signs included tachycardia with a heart rate of 116 beats/min, respiratory rate of 16 breaths/min, blood pressure of 116/84 mm Hg, temperature of 37.4°C, and oxygen saturation of 99% on room air. Her weight was 54.4 kg (50th percentile for age), height was 168 cm (75th percentile for age), body mass index (BMI) was 19.2 kg/m2 (27th percentile for age); she also had an increased arm span (174.5 cm) to height (168 cm) ratio (1.04) and a reduced upper segment (69 cm) to lower segment (99 cm) ratio (0.69), which were consistent with her diagnosis of Marfan syndrome.
Abdominal examination revealed epigastric tenderness and normal bowel sounds. She had a typical Marfanoid habitus, including enophthalmos, arachnodactyly, a positive thumb sign (thumbs protrude from clenched fists) (Figure 1), a positive wrist sign (the thumb and fifth digit overlap when grasping the contralateral wrist), pectus excavatum, and severe lumbar dextroscoliosis.

Figure 1. Positive ‘"thumb sign’" in patient’s left hand
Laboratory tests. Results of initial laboratory tests, including a complete blood cell count, a basic metabolic panel, liver function tests, an amylase test, a lipase test, and urinalysis, were normal. Urine pregnancy test results were negative.
After initial resuscitation with an intravenous (IV) bolus of normal saline, the patient was kept nil orally with maintenance IV fluids (0.45% sodium chloride with 5% dextrose). Abdominal radiographs revealed marked gastric distension with small bowel ileus, indicating possible gastric outlet obstruction or gastric volvulus (Figures 2 and 3). Contrast-enhanced computed tomography (CT) scans of her abdomen and pelvis showed severe dilatation of the stomach and the first and second parts of the duodenum and a collapsed distal small bowel (Figures 4 and 5). These findings were consistent with small bowel obstruction at the level of the mid or distal duodenum, possibly due to volvulus or superior mesenteric artery syndrome (SMAS). The radiographs also confirmed lumbar dextroscoliosis and severe pectus excavatum. The decision was made to perform an urgent laparotomy to relieve her intestinal obstruction.

Figure 2. Abdominal radiograph, anteroposterior view in erect posture, showing marked gastric distension with an air-fluid level and dextroscoliosis of the lumbar vertebrae.

Figure 3. Abdominal radiograph, left lateral decubitus view, showing marked distension and lumbar scoliosis.
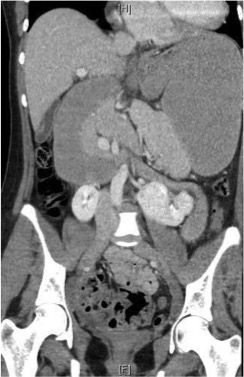
Figure 4. CT of the abdomen and pelvis, coronal view; arrows show severe dilatation of the stomach and the first and second parts of the duodenum, along with a collapsed distal small bowel.
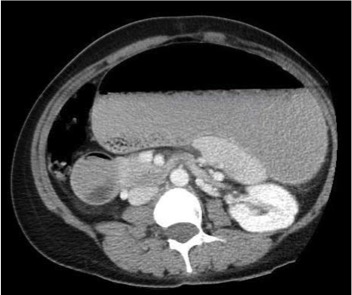
Figure 5. CT of the abdomen and pelvis, transverse view, showing severe dilatation of the stomach and the first and second parts of the duodenum, along with a collapsed distal small bowel.
Diagnosis and outcome of the case. Intraoperatively, a markedly distended duodenum and a collapsed bowel on the left side of the ligament of Treitz were noted, and the diagnosis of SMAS was established. The ligament of Treitz was divided; the duodenojejunal junction was fully mobilized so that the small bowel did not lie in the acute angle between the superior mesenteric artery (SMA) and the aorta, thereby relieving the obstruction. The patient tolerated the surgery well and had a brief, uneventful postoperative recovery. She remained asymptomatic in the long term after surgery.
Discussion. SMAS is a rare cause of mid or upper gastrointestinal tract obstruction due to compression of the third part of the duodenum between the SMA and the abdominal aorta.1-10 It was first described by von Rokitansky in 1842 and was subsequently found to be associated with orthopedic casting by Willet in 1878.1 In 1927, Wilkie described SMAS in a case series with 75 patients.3 Pediatric SMAS typically affects adolescents, with girls more often affected than boys. However, there have been rare reports of SMAS in infants, as well.6
The mechanism involves the loss of preduodenal fat and narrowing of the aortomesenteric angle (normal value, 25-60° with aortomesenteric distance of 10-28 mm; these values reduce to 6-15° and 2-8 mm, respectively, in SMAS). Consequently, entrapment of the duodenum occurs between the aorta and the SMA, resulting in obstruction, edema, and thickening of duodenal mucosa.9
The risk factors for development of SMAS include significant weight loss, hyperthyroidism, anorexia nervosa, paraplegia, orthopedic cast application, and spinal surgery.1,8 Our patient’s BMI was 19.2 kg/m2, and she did not have any of these risk factors. She had a known diagnosis of Marfan syndrome. This association has been described only once in the literature.11
Presenting symptoms of SMAS usually are those of small bowel obstruction, including nausea, vomiting, early satiety, abdominal pain, and anorexia. Acute, subacute, and chronic presentations have been described, with the median length of symptoms being 5 days.1,9 Other rare complications can include portal vein thrombosis5 and recurrent pregnancy loss.
In the majority of patients, the diagnosis of SMAS can be made via upper gastrointestinal tract radiographs, which may show dilatation of the stomach and duodenum proximal to the obstruction. Although a CT scan is more precise, it rarely can mimic volvulus or intestinal malrotation (as was seen in our case), and an accurate diagnosis may be made only at surgery.1 Selective SMA angiography has been used to precisely determine the aortomesenteric angle.2
Approximately 70% to 80% of patients with SMAS respond to conservative measures such as bowel decompression with nasojejunal tube placement past the obstruction site, restoration of fluid and electrolyte homeostasis, removal of body cast if applicable, calorie-dense oral feeds, knee-chest or right lateral decubitus feeding positions, and weight restoration.1,4 However, if these measures fail or if there is a diagnostic dilemma in a case of acute abdomen, surgical exploration should not be delayed. In addition to resection of the ligament of Treitz, which was done successfully in our case, other acceptable alternatives include gastrojejunostomy, Roux-en-Y duodenojejunostomy, and anterior transposition of the third part of the duodenum.2 The advantage of a ligament of Treitz division is that it eliminates the need for anastomosis and gut resection, thus avoiding the associated postoperative morbidities. The outcomes of these procedures are usually excellent, and patients start to tolerate oral feeds immediately.2
Conclusion. This is the second reported case of an association of SMAS and Marfan syndrome in an adolescent girl, in which her Marfanoid habitus placed her at a risk of SMAS. Also of note, the diagnosis of SMAS may elude imaging study results, emphasizing the importance of maintaining a high index of suspicion for timely recognition and treatment of SMAS, especially in presence of known risk factor(s).
Acknowledgement:
The authors acknowledge Jeffrey Chan, MD, Department of Pediatric Surgery, Jamaica Hospital Medical Center; Dakshayani Guttal, MD, Department of Pediatrics, Jamaica Hospital Medical Center; Rohit Pinto, MD, Department of Pediatrics, the Children’s Hospital at SUNY Downstate, Brooklyn; and Jayandra Sharma, MD, Division of Pediatric Cardiology, Jamaica Hospital Medical Center, for their contributions to the patient’s care. The authors also acknowledge Paul Joseph Simpson, MD, Department of Internal Medicine, Queens Hospital Center, for their editorial assistance in preparing the manuscript.
References:
- Biank V, Werlin S. Superior mesenteric artery syndrome in children: a 20-year experience. J Pediatr Gastroenterol Nutr. 2006;42(5):522-525.
- Javaid U, Mustafawi AR, Ahmed M; The superior mesenteric artery syndrome (SMAS): is it really a diagnostic dilemma? Ann Pediatr Surg. 2009;5(3):205-209.
- Wilkie DPD. Chronic duodenal ileus. Am J Med Sci. 1927; 173:643-649.
- Burrington JD. Superior mesenteric artery syndrome in children. Am J Dis Child. 1976;130(12):1367-1370.
- Rod J, Sarnacki S, Petit T, Ravasse P. Portal venous gas and thrombosis complicating superior mesenteric artery syndrome (Wilkie’s syndrome) in a child. J Pediatr Surg. 2010;45(4):826-829.
- Okugawa Y, Inoue M, Uchida K, et al. Superior mesenteric artery syndrome in an infant: case report and literature review. J Pediatr Surg. 2007;42(10): E5-E8.
- Iko BO, Monu JU, Orhue A, Sarkar SA. The superior mesenteric artery syndrome in pregnancy: a case resulting in recurrent pregnancy loss. Eur J Obstet Gynecol Reprod Biol. 1986;21(4):233-236.
- Tsirikos AI, Jeans LA. Superior mesenteric artery syndrome in children and adolescents with spine deformities undergoing corrective surgery. J Spinal Disord Tech. 2005;18(3):263-271.
- Feinberg AN. Case 1: duodenal compression and obstruction—superior mesenteric artery syndrome. Pediatr Rev. 1998;19(8):281-282.
- Lo CM, Lau HK, Kei SK. Superior mesenteric artery syndrome: an uncommon cause of abdominal pain mimicking gastroenteritis. Hong Kong J Emerg Med. 2008;15(4):235-239.
- Jain V, Singhal AK, Chithra R, Raghunaathan KD. Superior mesenteric artery syndrome: a rare complication in a child with Marfan syndrome. Arch Dis Child. 2013;98(10):754-755.