
Infectious Disease Emergencies: Part 2, Septic and Nonseptic Febrile Syndromes
ABSTRACT: The diagnosis of staphylococcal toxic shock syndrome (TSS) is largely clinical because Staphylococcus aureus is rarely recovered from blood cultures. Patients with staphylococcal TSS have fever, hypotension (initially presenting as orthostatic dizziness or syncope), and skin manifestations (diffuse erythroderma, pruritic maculopapular rash, and desquamation). Symptoms or history of present illness that are more suggestive of streptococcal TSS than of staphylococcal TSS include recent trauma, severe pain, and physical findings of soft tissue infections (ie, localized swelling and erythema, followed by ecchymosis and sloughing of skin). Another distinguishing feature of streptococcal TSS is that Streptococcus pyogenes is readily recovered from blood cultures.
Key words: staphylococcal toxic shock syndrome, streptoccal toxic shock syndrome
____________________________________________________________________________________________________________________________________________________
The diagnosis of many serious infectious diseases relies heavily on clinical suspicion, particularly in the early stages of the illness. In this 3-part series, we provide useful clues to the triage and diagnosis of these diseases.
Here we discuss staphylococcal toxic shock syndrome (TSS) and streptococcal TSS (Table). In a previous article (CONSULTANT, November 2010, page 473), the focus was on serious infections that present with rash and fever. In a coming issue, we will address CNS infections.
STAPHYLOCOCCAL TOXIC SHOCK SYNDROME
Overview. Staphylococcal TSS is caused by toxic shock syndrome toxin-1 and other enterotoxins that are produced by most methicillin-sensitive Staphylococcus aureus (MSSA) and methicillin-resistant S aureus (MRSA). There are 2 subcategories of staphylococcal TSS:
- Menstrual-related cases: classically associated with the use of highly absorbent tampons.
- Nonmenstrual-related cases: seen in a wide spectrum of clinical scenarios, including surgical and postpartum wound infections, mastitis, septorhinoplasty, sinusitis, osteomyelitis, arthritis, burns, cutaneous and subcutaneous lesions, respiratory tract infections (eg, following influenza), and enterocolitis.1-7
The incidence of menstrual-related cases of staphylococcal TSS has steadily declined since the withdrawal of highly absorbent tampons.8 Similarly, the case-fatality rate has paralleled this decline and is presently estimated to be about 1.8%.9 In contrast, nonmenstrual-related cases have a case-fatality rate of about 5%, which has remained steady throughout the years.
Clinical features. Patients with staphylococcal TSS have fever, hypotension (initially presenting as orthostatic dizziness or syncope), and skin manifestations (diffuse erythroderma, pruritic maculopapular rash, and desquamation). Other constitutional symptoms include chills, malaise, headache, pharyngitis, myalgias, fatigue, vomiting, diarrhea, and abdominal pain.10-12 In addition, cerebral ischemia and edema may also occur and manifest as somnolence, confusion, irritability or agitation, and hallucinations. 11-14 The CDC uses a case definition of TSS6,11,12 (ie, temperature of 39.9°C [102°F] or higher, hypotension, diffuse erythroderma, desquamation, and involvement of at least 3 organ systems) for epidemiological surveillance; however, this should not override clinical suspicion.

Diagnosis. The diagnosis is largely clinical, especially because S aureus is rarely recovered from blood cultures in patients with staphylococcal TSS. Wound sites, if present, may be cultured to aid in diagnosis (about 80% to 90% of patients have S aureus isolated from mucosal or wound sites),15 and isolates can then be tested for toxin production in research laboratories.
Treatment. Hospitalization is required. Treatment is chiefly directed toward supportive measures for hypotension, which can be refractory to large volumes of intravenous fluids, can persist for several days, and often leads to tissue ischemia and organ failure. Surgery may also prove beneficial if the clinical picture warrants such intervention.
Empiric antibiotic therapy consists of clindamycin (which can suppress toxin synthesis) and vancomycin.16 If cultures are isolated, the antibiotic regimen can be tailored specifically against MSSA (using clindamycin and oxacillin or nafcillin) or MRSA (using vancomycin or linezolid with or without clindamycin, depending on the susceptibilities).
STREPTOCOCCAL TOXIC SHOCK SYNDROME
Overview. TSS caused by group A streptococcus (GAS), or Streptococcus pyogenes, stems from severe, invasive infections, such as bacteremia, pneumonia, necrotizing fasciitis, and spontaneous gangrenous myositis, and is associated with acute onset of shock and organ failure. Like staphylococcal TSS, GAS TSS is mediated by exotoxins, most notably streptococcal pyrogenic exotoxins (SPE) A and B, of which SPE B predominates in the United States.17-20
According to the CDC, about 9000 to 11,500 cases of invasive GAS disease occur each year in the United States; streptococcal TSS accounts for 6% to 7% of these cases. The CDC also estimates that more than 50% of streptococcal TSS cases are fatal.10
Clinical features. Patients often present with nonspecific symptoms, such as fever, chills, myalgia, nausea, vomiting, and diarrhea, which are also associated with staphylococcal TSS.11,12 Potential neurological changes that may occur with GAS TSS or S aureus TSS include confusion, combativeness, and coma.11-14 Refractory hypotension is a classic feature of both GAS TSS and staphylococcal TSS.
Symptoms or history of present illness that are more suggestive of GAS TSS than of staphylococcal TSS include:
- Recent trauma.
- Severe pain.
- Physical findings of soft tissue infections (ie, localized swelling and erythema, followed by ecchymosis and sloughing of skin) (Figure 1).


Figure 1 – This rash in the pretibial area (A) was noted in a 44-year-old man with suspected streptococcal toxic shock syndrome. Following antibiotic therapy, the rash evolved into scaly, macular lesions that blistered and resolved with skin sloughing (B).
(Photographs courtesy of Mehdi Djekidel, MD, and Cynthia Piko, MD.)
Diagnosis. Another distinguishing feature of GAS TSS is that S pyogenes is readily recovered from blood cultures, in contrast to staphylococcal TSS, in which S aureus is rarely recovered from blood cultures. Overall, the features suggestive of GAS TSS are summarized in a clinical guideline developed by The Working Group on Severe Streptococcal Infections. The criteria for diagnosis consist of isolation of GAS from a normally sterile site and hypotension, in addition to 2 or more of the following21:
- Renal impairment.
- Coagulopathy.
- Liver involvement.
- Adult respiratory distress syndrome.
- Erythematous macular rash (may desquamate).
- Soft tissue necrosis (Figure 2).
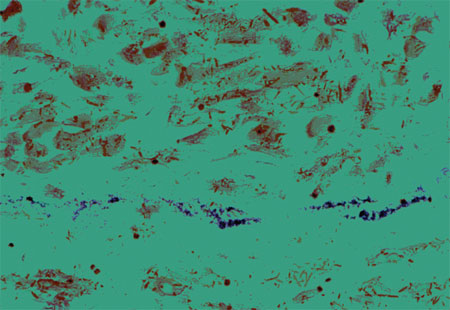 Figure 2 – A sample of muscle tissue from a patient with group A streptococcal necrotizing fasciitis/myonecrosis shows an abundance of gram-positive cocci and extensive muscle destruction. The patient was a 65-year-old man in whom toxic shock syndrome developed; he died 24 hours after admission. (Photomicrograph courtesy of Dennis L. Stevens, PhD, MD.)
Figure 2 – A sample of muscle tissue from a patient with group A streptococcal necrotizing fasciitis/myonecrosis shows an abundance of gram-positive cocci and extensive muscle destruction. The patient was a 65-year-old man in whom toxic shock syndrome developed; he died 24 hours after admission. (Photomicrograph courtesy of Dennis L. Stevens, PhD, MD.)
Treatment. The treatment of GAS TSS is similar to that of staphylococcal TSS. Patients with suspected GAS TSS require hospitalization, and treatment is largely directed at supportive measures for hypotension. Surgery is necessary if soft tissue infection is present.
Empiric antibiotic therapy consists of clindamycin in addition to a combination drug containing a penicillin plus β-lactamase inhibitor (ie, ticarcillin/clavulanate or piperacillin/ tazobactam), since clindamycin-resistant isolates are known to occur (more so in Europe than in the United States).22,23 However, clindamycin remains the drug of choice for treatment of GAS TSS. Among its advantages over penicillin-containing antibiotics are:
- Suppression of the synthesis of bacterial toxins.24-26
- Facilitation of phagocytosis of S pyogenes.25
- Longer postantibiotic effect.
1. Bartlett P, Reingold AL, Graham DR, et al. Toxic shock syndrome associated with surgical wound infections. JAMA. 1982;247:1448-1450.
2. Ferguson MA, Todd JK. Toxic shock syndrome associated with Staphylococcus aureus sinusitis in children. J Infect Dis. 1990;161:953-955.
3. Dann EJ, Weinberger M, Gillis S, et al. Bacterial laryngotracheitis associated with toxic shock syndrome in an adult. Clin Infect Dis. 1994; 18:437-439.
4. Morrison VA, Oldfield EC 3rd. Postoperative toxic shock syndrome. Arch Surg. 1983;118:791-794.
5. Paterson MP, Hoffman EB, Roux P. Severe disseminated staphylococcal disease associated with osteitis and septic arthritis. J Bone Joint Surg Br. 1990;72:94-97.
6. Reingold AL, Hargrett NT, Dan BB, et al. Nonmenstrual toxic shock syndrome: a review of 130 cases. Ann Intern Med. 1982;96(6, pt 2):871-874.
7. Kotler DP, Sandkovsky U, Schlievert PM, Sordillo EM. Toxic shock-like syndrome associated with staphylococcal enterocolitis in an HIV-infected man. Clin Infect Dis. 2007;44:e121-e123.
8. Centers for Disease Control. Reduced incidence of menstrual toxic-shock syndrome—United States 1980-1990. MMWR. 1990;39:421-423.
9. Hajjeh RA, Reingold A, Weil A, et al. Toxic shock syndrome in the United States: surveillance update, 1979-1996. Emerg Infect Dis. 1999;5:807-810.
10. Centers for Disease Control and Prevention. Toxic shock syndrome. October 24, 2005. Accessed October 18, 2010.
11. Wharton M, Chorba TL, Vogt RL, et al. Case definitions for public health surveillance. MMWR Recomm Rep. 1990;39(RR-13):1-43.
12. Centers for Disease Control and Prevention. Case definitions for infectious conditions under public health surveillance. MMWR Recomm Rep. 1997;46(RR-10):1-55.
13. Barrett JA, Graham DR. Toxic shock syndrome presenting as encephalopathy. J Infect. 1986;12:276-278.
14. Smith DB, Gulinson J. Fatal cerebral edema complicating toxic shock syndrome. Neurosurgery. 1988;22:598-599.
15. Davis JP, Osterholm MT, Helms CM, et al. Tri-state toxic-shock syndrome study. II. Clinical and laboratory findings. J Infect Dis. 1982;145:441-448.
16. Schlievert PM, Kelly JA. Clindamycin-induced suppression of toxic-shock syndrome—associated exotoxin production. J Infect Dis. 1984;149:471.
17. Stevens DL, Tanner MH, Winship J, et al. Severe group A streptococcal infections associated with a toxic shock-like syndrome and scarlet fever toxin A. N Engl J Med. 1989;321:1-7.
18. Schwartz B, Facklam RR, Brieman RF. Changing epidemiology of group A streptococcal infection in the USA. Lancet. 1990;336:1167-1171.
19. Hauser AR, Stevens DL, Kaplan EL, Schlievert PM. Molecular analysis of pyrogenic exotoxins from Streptococcus pyogenes isolates associated with toxic shock-like syndrome. J Clin Microbiol. 1991; 29:1562-1567.
20. Musser JM, Hauser AR, Kim MH, et al. Streptococcus pyogenes causing toxic-shock-like syndrome and other invasive diseases: clonal diversity and pyrogenic exotoxin expression. Proc Natl Acad Sci U S A. 1991;88:2668-2672.
21. Defining the group A streptococcal toxic shock syndrome. Rationale and consensus definition. The Working Group on Severe Streptococcal Infections. JAMA. 1993;269:390-391.
22. Richter SS, Heilmann KP, Beekmann SE, et al. Macrolide-resistant Streptococcus pyogenes in the United States, 2002-2003. Clin Infect Dis. 2005;41: 599-608.
23. Gooskens J, Neeling AJ, Willems RJ, et al. Streptococcal toxic shock syndrome by an iMLS resistant M type 77 Streptococcus pyogenes in the Netherlands. Scand J Infect Dis. 2005;37:85-89.
24. Stevens DL, Maier KA, Mitten JE. Effect of antibiotics on toxin production and viability of Clostridium perfringens. Antimicrob Agents Chemother. 1987;31:213-218.
25. Gemmell CG, Peterson PK, Schmeling D, et al. Potentiation of opsonization and phagocytosis of Streptococcus pyogenes following growth in the presence of clindamycin. J Clin Invest. 1981;67:1249-1256.
26. Mascini EM, Jansze M, Schouls LM, et al. Penicillin and clindamycin differentially inhibit the production of pyrogenic exotoxins A and B by group A streptococci. Int J Antimicrob Agents. 2001;18:
395-398.