More than half of travelers to the developing world experience a health-related problem during their trip, with 8% requiring medical attention on their return because of persistent symptoms.1 The GeoSentinel database, a collaborative effort among 31 travel medicine clinics on 6 different continents, suggests that the most common diagnoses in these persons continue to be malaria (24%), dengue fever (DF) (6%), acute traveler’s diarrhea (4%), and typhoid fever (2%).2 In recent years, however, the changing epidemiology of several pathogens has posed new risks to travelers. Among these are avian influenza, novel H1N1 (swine) influenza, multidrug-resistant tuberculosis (MDRTB), chikungunya virus (CHIKV) infection (ie, chikungunya fever), leishmaniasis, and DF.
In our 2-part series, we discuss these emerging infections and summarize new travel requirements and vaccine recommendations. Here we focus on CHIKV infection, leishmaniasis, and DF; in a previous article (Travel Medicine: Emerging Pathogens and New Recommendations, CONSULTANT, September 2009, page 549), we discussed avian influenza, novel H1N1 influenza, and MDR-TB.
CHIKUNGUNYA FEVER
CHIKV, an arbovirus transmitted by the Aedes aegypti mosquito, was first identified in Tanzania in 1953.3 Chikungunya is derived from the local word kungunyala meaning “contorted,” and refers to the severe joint pain experienced by infected patients. 4
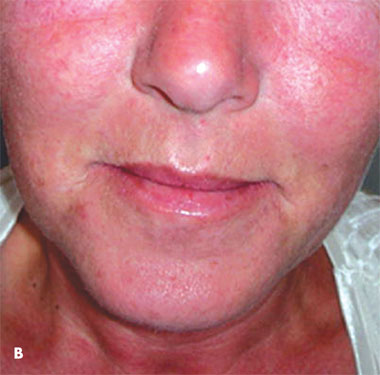
 Acute infection is characterized by fever; headache; myalgias; and a subacute, bilateral polyarthralgia that typically affects the distal joints of the fingers, toes, ankles, and wrists.5 Rash is frequently observed; among 47 French patients returning from the Indian Ocean islands with CHIKV infection, 24 noted an evanescent pruritic rash over the face, trunk, or extremities accompanied by edema (Figure 1).6 Among 46 persons in this group of travelers, less common clinical manifestations were bilateral conjunctivitis in 2 patients (4%) and large joint effusions in 7 patients (15%). Common laboratory findings include elevation of liver and muscle enzyme levels, mild thrombocytopenia, and leukopenia. Hematological abnormalities in the acute phase may be associated with bleeding. Affected patients may suffer from a protracted illness characterized by persistent polyarthralgias and a limited ability to perform activities of daily living. Tenosynovitis also may exacerbate these late-stage symptoms.6,7
Acute infection is characterized by fever; headache; myalgias; and a subacute, bilateral polyarthralgia that typically affects the distal joints of the fingers, toes, ankles, and wrists.5 Rash is frequently observed; among 47 French patients returning from the Indian Ocean islands with CHIKV infection, 24 noted an evanescent pruritic rash over the face, trunk, or extremities accompanied by edema (Figure 1).6 Among 46 persons in this group of travelers, less common clinical manifestations were bilateral conjunctivitis in 2 patients (4%) and large joint effusions in 7 patients (15%). Common laboratory findings include elevation of liver and muscle enzyme levels, mild thrombocytopenia, and leukopenia. Hematological abnormalities in the acute phase may be associated with bleeding. Affected patients may suffer from a protracted illness characterized by persistent polyarthralgias and a limited ability to perform activities of daily living. Tenosynovitis also may exacerbate these late-stage symptoms.6,7
 Initially limited to Africa and Southeast Asia, CHIKV has recently spread to territories in the western and eastern Indian Ocean and India.8 In 2006, outbreaks of chikungunya fever in the Indian Ocean islands were attributed to an emerging vector, Aedes albopictus.9 Affected islands included the Comoros, Mauritius, the Seychelles, Madagascar, Mayotte, and Réunion. In Réunion, 265,000 clinical cases occurred among 770,000 inhabitants (34%), resulting in 237 deaths. That year, India reported an estimated 1.3 million cases10 and the global number of cases was close to 2 million.8 From 1991 to 2005, only 7 imported cases of CHIKV infection were identified in the United States, compared with 37 cases from 2005 through late September 2006.11
Initially limited to Africa and Southeast Asia, CHIKV has recently spread to territories in the western and eastern Indian Ocean and India.8 In 2006, outbreaks of chikungunya fever in the Indian Ocean islands were attributed to an emerging vector, Aedes albopictus.9 Affected islands included the Comoros, Mauritius, the Seychelles, Madagascar, Mayotte, and Réunion. In Réunion, 265,000 clinical cases occurred among 770,000 inhabitants (34%), resulting in 237 deaths. That year, India reported an estimated 1.3 million cases10 and the global number of cases was close to 2 million.8 From 1991 to 2005, only 7 imported cases of CHIKV infection were identified in the United States, compared with 37 cases from 2005 through late September 2006.11
 CHIKV infection should be a consideration in travelers with fever and arthralgias who have recently returned from areas where CHIKV is transmitted. Acute- and convalescentphase serum specimens can be submitted to the CDC for testing through state health departments. Unfortunately, no vaccine or specific antiviral treatment exists. Therapy consists of supportive care, including rest, fluids, and antipyretics. Late-stage symptoms have demonstrated a dramatic response to short-term corticosteroid therapy. The CDC suggests that infected persons should be protected from further mosquito exposure by staying indoors or under a mosquito net during the first few days of illness, thus limiting propagation of the transmission cycle.12 Recommendations for prevention are detailed in the Table.
CHIKV infection should be a consideration in travelers with fever and arthralgias who have recently returned from areas where CHIKV is transmitted. Acute- and convalescentphase serum specimens can be submitted to the CDC for testing through state health departments. Unfortunately, no vaccine or specific antiviral treatment exists. Therapy consists of supportive care, including rest, fluids, and antipyretics. Late-stage symptoms have demonstrated a dramatic response to short-term corticosteroid therapy. The CDC suggests that infected persons should be protected from further mosquito exposure by staying indoors or under a mosquito net during the first few days of illness, thus limiting propagation of the transmission cycle.12 Recommendations for prevention are detailed in the Table.

CUTANEOUS LEISHMANIASIS
Leishmania species are intracellular protozoal parasites transmitted by the sandfly, most often in a rural setting. A wide spectrum of clinical manifestations, such as ulcerative skin lesions, mucocutaneous involvement, and visceral disease (kala-azar), exist and are characterized as either Old World (southern Europe, Middle East, Asia, and Africa) or New World (Latin America). Cutaneous leishmaniasis (CL) is endemic to more than 70 countries, with 90% of cases occurring in Afghanistan, Algeria, Brazil, Pakistan, Peru, Saudi Arabia, and Syria.13 Global incidence is increasing, with an estimated 1.5 to 2 million new cases each year, resulting in more than 70,000 deaths.14
Travel to regions of Central and South America where Leishmania is endemic has resulted in an increasing number of imported cases of New World CL in Europe. Between 1995 and 2003, the number of cases increased 3-fold in the United Kingdom.
Similarly, between 1990 and 2000, the number of imported cases doubled in the Netherlands.13 Old World CL, most often associated with Leishmania major or Leishmania tropica, has been identified among US military personnel deployed to Afghanistan, Iraq, and Kuwait. 15
 From June 2003 to April 2004, more than 600 cases of Old World CL were diagnosed among American soldiers participating in Operation Iraqi Freedom. When cultures could be obtained (n = 308) from biopsies of skin lesions, L major was the pathogen in 99% of cases.16 CL is a chronic disease with lesions appearing within 1 to 7 months of exposure.17 Typically, an initial lesion develops at the site of the sandfly bite as a small, erythematous papule. Progressive ulceration follows within 2 weeks to 6 months of infection. Ulcerated lesions are typical of infection caused by New World species and L major (Figure 2).
From June 2003 to April 2004, more than 600 cases of Old World CL were diagnosed among American soldiers participating in Operation Iraqi Freedom. When cultures could be obtained (n = 308) from biopsies of skin lesions, L major was the pathogen in 99% of cases.16 CL is a chronic disease with lesions appearing within 1 to 7 months of exposure.17 Typically, an initial lesion develops at the site of the sandfly bite as a small, erythematous papule. Progressive ulceration follows within 2 weeks to 6 months of infection. Ulcerated lesions are typical of infection caused by New World species and L major (Figure 2).
More severe cutaneous disease may spread locally or hematogenously to involve deeper tissues. In Latin America, most such cases are caused by Leishmania braziliensis and Leishmania amazonensis.18 A detailed review of therapeutic options for CL has been provided elsewhere.13 Intralesional and parenteral pentavalent antimonials—sodium stibogluconate and meglumine antimoniate—have been used successfully, but serious adverse effects, such as myalgias, renal failure, hepatotoxicity, and cardiotoxicity, may occur.19 In the United States, sodium stibogluconate is available for parenteral use under an investigational drug protocol by contacting the CDC (telephone, 404-639-3670). Alternative treatment regimens have met with varying success, including amphotericin B and its lipid formulations, pentamidine, and miltefosine.13 Oral azoles (eg, ketoconazole, fluconazole, topical agents (eg, paromomycin cream), and thermotherapy have also been used. Personal protection against sandflies is necessary for travelers.20
The CDC recommendations for prevention are detailed in the Table.
DENGUE FEVER
DF and dengue hemorrhagic fever (DHF) are caused by 4 related but antigenically distinct dengue virus serotypes of the virus family Flaviviridae. DF is a self-limited disease characterized by the sudden onset of fever, severe headache, myalgias, and arthralgias, which are often accompanied by a maculopapular rash. DHF is a more severe disease with a mortality rate between 1% and 50% in developed and developing countries, respectively.21 It occurs 4 to 7 days after dengue virus infection and is heralded by capillary leakage and hemorrhagic complications. Neutropenia, elevated liver enzyme levels, and disseminated intravascular coagulation are also common. One of the most important risk factors for DHF is previous dengue virus infection.22 Therefore, the risk to first-time international travelers from areas where the disease is not endemic is low, but the risk increases with subsequent travel.
The primary vector of dengue virus is A aegypti, although infection associated with A albopictus23 also has been reported. Most cases of DF and DHF have been reported in Asia, but in the late 1980s and early 1990s, epidemics occurred in Southeast Asia, the Pacific Islands, the Caribbean, and Latin America.24 Over the past few years, DF has become endemic to most tropical countries of the South Pacific, Asia, the Caribbean, the Americas, and Africa. Dengue virus is the most common cause of arboviral disease in the world, accounting for 50 million to 100 million cases and more than 22,000 deaths annually.25 The marked increase in DF over the past 2 decades in areas where the disease is endemic also has resulted in increased infection rates among travelers. DF and DHF have been diagnosed in up to 16% of febrile travelers returning from the tropics, a 3-fold increase since 1990.26
From 1977 to 2004, 864 cases of DF were reported in the United States among returning travelers.27 Rarely, these infected travelers can serve as a source for DF transmission when returning to an A aegypti—infested or A albopictus— infested area. This phenomenon was demonstrated in Hawaii in 2001, when the arrival of a single viremic traveler from the South Pacific resulted in a limited local outbreak.28 A aegypti, a daytime feeder, is found most frequently in or near human habitations. Mosquito breeding sites include artificial water containers, such as discarded tires, uncovered water storage barrels, buckets, and cisterns. Extensive public health measures have been taken to limit these potential breeding sites. For travelers, the most effective preventive measure is the use of insect repellents containing N,N-diethylmeta-toluamide (DEET) and permethrin-impregnated protective clothing.29 Because the transmission risk is highest during the day, the utility of bed nets at night is limited. Travelers to areas where DF is endemic and epidemic should take precautions to avoid mosquito bites as detailed in the Table.
TRAVEL REQUIREMENTS AND VACCINE RECOMMENDATIONS
In 2008, yellow fever vaccination requirements expanded to travelers to Costa Rica, Argentina, Paraguay, Bolivia, and Brazil. Specifics may be obtained by reviewing The Yellow Book, CDC Health Information for International Travel 2008.30 A new International Certificate of Vaccination or Prophylaxis (ICVP) was issued in December 2007 and should be used to record yellow fever vaccine administration. Health care practitioners should replace older versions with the current ICVP whenever possible.
In October 2007, the tetravalent meningococcal polysaccharide-protein conjugate vaccine (MCV4), conferring protection against Neisseria meningitidis serogroups A, C, Y, and W-135, was approved for use in children aged 2 to 10 years.31 The Advisory Committee on Immunization Practices (ACIP) recommends the use of meningococcal vaccine for persons who travel to or reside in countries in which N meningitidis is hyperendemic or epidemic, particularly if contact with the local population will be prolonged. MCV4 is preferred and may now be used among persons aged 2 to 55 years. MPSV4, a tetravalent meningococcal polysaccharide vaccine, remains the recommended vaccine among persons older than 55 years who travel to regions in which N meningitidis is prevalent.32 In 2006, an outbreak of mumps in the United States prompted revised recommendations for vaccination. Presently, according to the ACIP, adequate mumps vaccination for international travelers now consists of 2 doses of live virus vaccine instead of 1 dose.33
Routine adult vaccine guidelines have been updated to include varicellazoster vaccination of adults 60 years and older who have evidence of past varicella immunity. Evidence of past varicella immunity is described in the 2008 ACIP Adult Immunization Schedule.34 All adults without evidence of immunity to varicella should receive 2 doses of single-antigen varicella vaccine unless they have a medical contraindication.
CONCLUSION
Because 40 million Americans travel or work abroad annually,35 physicians should be prepared to provide pre-travel counseling for their patients. To provide comprehensive care, clinicians must maintain a working knowledge of emerging pathogens and travel vaccination recommendations. Travel medicine experts and dedicated Web sites maintained by the CDC and the World Health Organization can provide additional valuable information.