
Disseminated Histoplasmosis
 A 38-year-old man had fever and fatigue for the past 6 days and tenderness in the left upper abdominal quadrant for the past 3 days. He also had a facial butterfly rash that had been present for 10 years and a 1-year history of lupus nephritis, treated with prednisone and mycophenolate. He denied respiratory complaints or recent weight loss.
A 38-year-old man had fever and fatigue for the past 6 days and tenderness in the left upper abdominal quadrant for the past 3 days. He also had a facial butterfly rash that had been present for 10 years and a 1-year history of lupus nephritis, treated with prednisone and mycophenolate. He denied respiratory complaints or recent weight loss.
The white blood cell (WBC) count was 6500/μL; hemoglobin level, 12.9 g/dL; and platelet count, 122,000/μL. The aspartate aminotransferase level was normal; the alanine aminotransferase level was slightly elevated at 155 U/L. Anti-DNA antibody titer was negative. C3 and C4 levels were normal. Results of blood, sputum, stool, and urine cultures were all negative.
 Chest radiograph was normal. Results of bronchoscopy with bronchoalveolar lavage showed fungal organisms within histiocytes, consistent with Histoplasma species. The urine Histoplasma antigen result was greater than 6.4; the yeast antibody titers were also positive at 1:256.
Chest radiograph was normal. Results of bronchoscopy with bronchoalveolar lavage showed fungal organisms within histiocytes, consistent with Histoplasma species. The urine Histoplasma antigen result was greater than 6.4; the yeast antibody titers were also positive at 1:256.
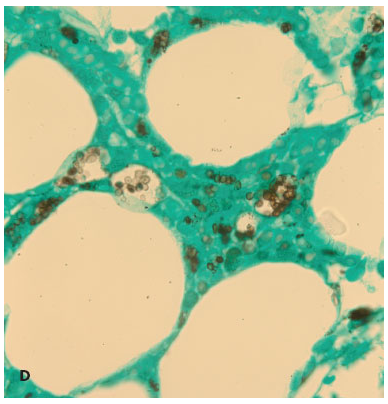
After the platelet count dropped to 20,000/μL and neutropenia developed (absolute neutrophil count, 879/μL), a bone marrow biopsy was performed. Results showed histiocytes containing yeast cells on Wright-Giemsa (A and B), periodic acid-Schiff (C), and Grocott-Gomori methenamine silver (D) staining methods. These findings were consistent with histoplasma and were confirmed with bone marrow culture growth of Histoplasma capsulatum.
be found worldwide, histoplasma is endemic to certain regions of the Americas, Asia, and Africa.1 The mycosis is more common in men; the mean age reported in one study was 55 years.2 The clinical presentation ranges from a mild flu-like illness to a rapidly progressive disseminated disease and varies according to the host’s immunity and the size of the inoculum.2 Fever, dyspnea, pleurisy, and weight loss are frequently reported. The most commonly involved tissues are the lung, liver, and bone marrow.3
Maintain a high level of suspicion for histoplasma in patients who live in regions where the disease is endemic and who present with fever, bone marrow suppression, and elevated liver enzyme levels, especially if the patient is immunosuppressed.2 Symptoms may mimic a lupus flare, or they may be masked by the use of corticosteroids.3 Measurement of anti-dsDNA and complement components may determine whether the patient has a lupus flare.4
 The treatment of choice for disseminated histoplasma is liposomal amphotericin B for 1 to 2 weeks, followed by oral itraconazole for 1 year.5 Periodic measurement of urine antigen levels during therapy is recommended, although blood cultures may provide a better measure of antifungal effect.6 This patient received itraconazole without liposomal amphotericin B, because of his markedly decreased renal function. His fever resolved within a few days of starting treatment. After a month, his WBC and platelet counts stabilized and he was discharged.
The treatment of choice for disseminated histoplasma is liposomal amphotericin B for 1 to 2 weeks, followed by oral itraconazole for 1 year.5 Periodic measurement of urine antigen levels during therapy is recommended, although blood cultures may provide a better measure of antifungal effect.6 This patient received itraconazole without liposomal amphotericin B, because of his markedly decreased renal function. His fever resolved within a few days of starting treatment. After a month, his WBC and platelet counts stabilized and he was discharged.
1. Ceccato F, Gongora V, Zunino A, et al. Unusual manifestation of histoplasmosis in connective tissue diseases. Clin Rheumatol. 2007;26: 1717-1719.
2. Assi MA, Sandid MS, Baddour LM, et al. Systemic histoplasmosis: a 15-year retrospective institutional review of 111 patients. Medicine (Baltimore). 2007;86:162-169.
3. Hansen KE, St Clair EW. Disseminated histoplasmosis in systemic lupus erythematosus: case report and review of the literature. Semin Arthritis Rheum. 1998;28:193-199.
4. Swaak AJ, Groenwold J, Bronsveld W. Predictive value of complement profiles and anti-dsDNA in systemic lupus erythematosus. Ann Rheum Dis. 1986;45:359-366.
5. Wheat LJ, Freifeld AG, Kleiman MB, et al. Clinical practice guidelines for the management of patients with histoplasmosis: 2007 update by the Infectious Diseases Society of America. Clin Infect Dis. 2007;45:807-825.
6. Wheat LJ, Connolly P, Haddad N, et al. Antigen clearance during treatment of disseminated histoplasmosis with itraconazole versus fluconazole in patients with AIDS. Antimicrob Agents Chemother. 2002;46:248-250.