
Appendicitis With Bowel Malrotation
 A 41-year-old woman presented to the emergency department with abdominal pain and vomiting of 1 week's duration. She had a history of surgery for bowel malrotation at age 11 days.
A 41-year-old woman presented to the emergency department with abdominal pain and vomiting of 1 week's duration. She had a history of surgery for bowel malrotation at age 11 days.
The patient had pain and tenderness in the left lower quadrant. White blood cell count was 9100/µL (normal, 4200 to 7500/µL) with a left shift (neutrophils, 82%). A pregnancy test was negative. Lipase and amylase levels were normal. Microscopic examination of urine showed few bacteria.

A CT scan of the abdomen and pelvis with oral and intravenous contrast revealed a 5-cm abscess (a) on the left side of the abdomen (A). Adjacent images showed tubular extensions of the abscess, one of which likely represented the appendix. Of note, jejunal bowel loops can be identified by their frond-like appearance on the right side of the abdomen (A, arrow). Normally, the duodenum crosses the midline between the aorta (Ao) and the superior mesenteric artery (S)--a more cephalad image reveals that the most medial extent of the duodenum does not cross the midline (B, arrow). A CT scan performed 6 months earlier during an evaluation for renal stones showed no abscess. Scout view from the prior CT scan demonstrated partially air-filled colon only on the left side of the abdomen (C).
 Joel M. Schwartz, MD, of Elmsford, NY, reports that prompt surgical exploration revealed massive adhesions. Small and large bowel loops were dissected away, and the abscess was drained. The appendix was identified and resected. Bacterial culture of the abscess was positive for Escherichia coli. The postoperative course was uneventful.
Joel M. Schwartz, MD, of Elmsford, NY, reports that prompt surgical exploration revealed massive adhesions. Small and large bowel loops were dissected away, and the abscess was drained. The appendix was identified and resected. Bacterial culture of the abscess was positive for Escherichia coli. The postoperative course was uneventful.
The differential diagnosis of nontraumatic left lower quadrant pain is extensive. Possible causes may include infection, calculi, ischemia, infarction, torsion, hemorrhage, obstruction, and benign or malignant neoplasm. These processes can affect the bowel, mesentery, and ureter and the ovary, fallopian tube, and uterus in females. Disease of a ptotic left kidney can also present with left lower quadrant symptoms.
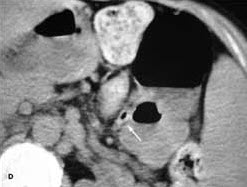 Appendicitis usually presents with right lower quadrant symptoms that occasionally start or remain in the midline. Inflamed elongated appendices can mimic pelvic pathology because of their caudal extent. In patients with malrotation, the small and large bowels do not undergo their normal development and fixation. The small bowel remains on the right side of the abdomen, while the large bowel and appendix are on the left (D, arrow, prior CT scan of same patient). Patients with malrotation only have a nonrotated bowel. In patients with situs inversus, all the abdominal organs are on the opposite side of normal. Patients who have situs inversus totalis have all their abdominal and thorax structures on the "wrong" side.
Appendicitis usually presents with right lower quadrant symptoms that occasionally start or remain in the midline. Inflamed elongated appendices can mimic pelvic pathology because of their caudal extent. In patients with malrotation, the small and large bowels do not undergo their normal development and fixation. The small bowel remains on the right side of the abdomen, while the large bowel and appendix are on the left (D, arrow, prior CT scan of same patient). Patients with malrotation only have a nonrotated bowel. In patients with situs inversus, all the abdominal organs are on the opposite side of normal. Patients who have situs inversus totalis have all their abdominal and thorax structures on the "wrong" side.
Patients with malrotation or situs inversus present with atypical symptoms because of the abnormal location of internal organs, such as in this patient, in whom the appendix is on the left. Clues can be found in the history--as in this case--as well as in the physical examination. For instance, in patients with situs inversus, percussion of the abdomen reveals that the liver is on the left side. Radiography with exquisite attention to labeling is diagnostic. Bowel malrotation can be suggested on plain film or CT; barium studies are confirmatory.