
What’sYour Diagnosis?
HISTORY
Ten-month-old girl with swelling of the left knee of 7 weeks’ duration. Unable to bear weight on the left leg for the past 2 weeks. No fever or history of trauma to the area. Infant has good appetite for breast milk and formula, but possible malaise. Infant born at full term via cesarean delivery because of cephalopelvic disproportion. No complications or extended hospital course. Growth and development, normal. Unremarkable family history. No prior surgeries.
PHYSICAL EXAMINATION
Vital signs, normal. Proximal intraphalangeal joint swelling, erythema, and warmth of the third digit of the left hand and minimal swelling and erythema of the left knee. Passive range of motion of both knee and interphalangeal joints slightly decreased relative to contralateral joints on flexion and extension. Patient resisted bearing weight with support and exhibited some favoring toward the right hand. Mild lymphadenopathy and mild hepatosplenomegaly noted. No other abnormalities.
LABORATORY INVESTIGATIONS
White blood cell count, 10,600/μL (75% segmented neutrophils, 25% lymphocytes); hemoglobin level, 12.1 g/dL; platelet count, 465,000/mL. Erythrocyte sedimentation rate, 23 mm/h (normal, 0 to 20 mm/h), and C-reactive protein level, 0.95 mg/L (normal, less than 0.5 mg/L). Antinuclear antibodies direct, 140 units/mL (negative, 0 to 99; equivocal, 100 to 120; positive, greater than 120). Mild anemia noted. Angiotensinconverting enzyme level, normal. Lyme and antistreptolysin O titers, negative.
IMAGING
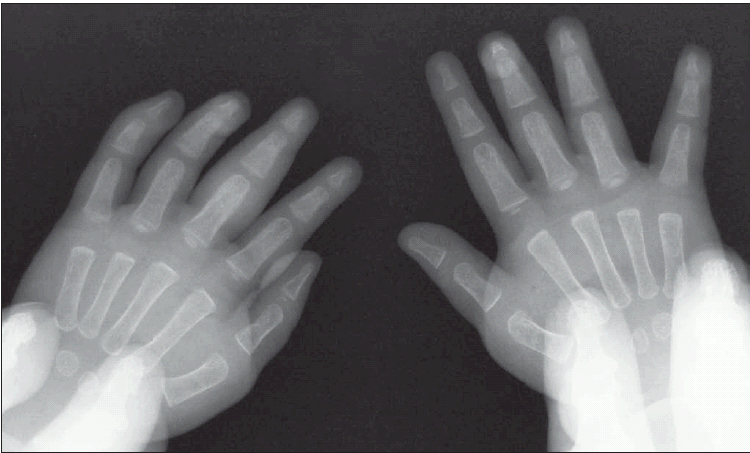
Radiograph of hands is shown.
WHAT’S YOUR DIAGNOSIS?
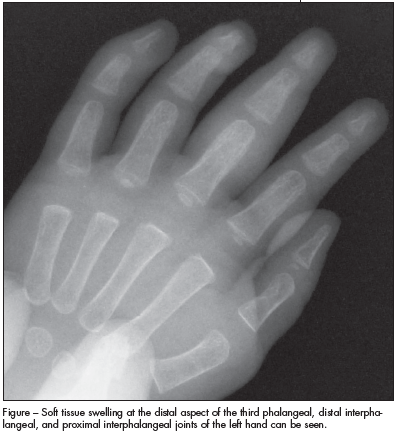
ANSWER: JUVENILE IDIOPATHIC ARTHRITISThe radiograph showed soft tissue swelling at the distal aspect of the third phalangeal, distal interphalangeal, and proximal interphalangeal joints of the left hand (Figure). There were no bony abnormalities or joint-space widening. Radiographs of the left knee showed mild swelling and no fracture or dislocation. These findings suggested a diagnosis of juvenile idiopathic arthritis (JIA). The laboratory test results ruled out other possible causes of arthritis and arthralgia, including Lyme disease, systemic lupus erythematosus, and septic arthritis
JIA: AN OVERVIEW
JIA, previously known as juvenile rheumatoid arthritis,1 is characterized by joint inflammation and stiffness of more than 6 weeks’ duration in a child 16 years or younger in whom other diagnoses have been ruled out. The peak incidence is between 1 and 3 years of age.2 JIA is the most common type of arthritis in children, with an estimated prevalence of 20 to 150 cases per 100,000 children; it generally affects girls more than boys by a ratio of 2:1.
The immunological cascade involved in JIA is thought to be initiated by the presentation of antigens to T lymphocytes by antigen-presenting cells.3 Cytokine release leads to the destruction of normal healthy cartilage by the inflamed articular cells and fluid. Inflammation causes erythema, swelling warmth, and soreness in the affected joints. JIA is not believed to be inherited.
Patients often have persistent joint swelling and pain that is typically worse in the morning or after awakening from a nap. However, joint pain may be absent in young children with JIA or these children may be unable to communicate their pain. Range of motion may be limited. JIA is often preceded by an acute febrile illness weeks to months before the joint manifestation, although that was not the case in this patient. In about one-third of patients, 1 or a few joints, most often ankles and knees, are involved.4
The 3 major types of JIA are characterized by certain signs and symptoms within the first 6 months of illness:
- Oligoarticular JIA—as seen in this patient—involves fewer than 5 joints and is more likely to be associated
- with a positive antinuclear antibody titer than the other types of JIA.5
- Polyarticular JIA involves 5 or more joints; rheumatoid factor may be positive.
- Systemic JIA may involve arthritis of 1 or multiple joints; patients may have fever, a pink (salmon-colored) rash, lymphadenopathy, and hepatosplenomegaly, which overshadow joint inflammation.
On radiographic studies, the fingers are typically involved in monarticular or oligoarticular JIA, whereas the entire hand is affected in those with polyarticular JIA.6
 Generalized lymphadenopathy is more common and the course of the disease is more unpredictable in children with JIA than in adults with rheumatoid arthritis. In children with disease of acute febrile onset, multiple joint involvement, and a positive rheumatoid factor, crippling deformities are more likely to develop.7 The primary morbidity associated with JIA is idiopathic inflammatory eye disease. Uveitis occurs in 10% to 30% of children with arthritis and is usually asymptomatic.8
Generalized lymphadenopathy is more common and the course of the disease is more unpredictable in children with JIA than in adults with rheumatoid arthritis. In children with disease of acute febrile onset, multiple joint involvement, and a positive rheumatoid factor, crippling deformities are more likely to develop.7 The primary morbidity associated with JIA is idiopathic inflammatory eye disease. Uveitis occurs in 10% to 30% of children with arthritis and is usually asymptomatic.8
OUTCOME IN THIS PATIENT
The infant was referred to pediatric rheumatology and treated with intra-articular corticosteroid joint injections. She eventually required subcutaneous methotrexate injections to control the inflammation. She was also referred to pediatric ophthalmology and will be evaluate every 6 months for any signs of uveitis.