
Peer Reviewed
Urticaria Secondary to Monoethanolamine Sensitivity
AUTHOR:
John Chin, MD
Commander, Submarine Squadron 6, Medical Department, Norfolk, Virginia
CITATION:
Chin J. Urticaria secondary to monoethanolamine sensitivity. Consultant360. 2016;56(7):651-652.
A 20-year-old, otherwise healthy US Navy midshipman experienced an acute pruritic eruption over both arms 6 hours into a submarine cruise (Figure 1). He denied any respiratory or cardiac distress and had no known allergies. He initially had been given 50 mg of diphenhydramine, followed by a second dose several hours later, when the symptoms failed to resolve.

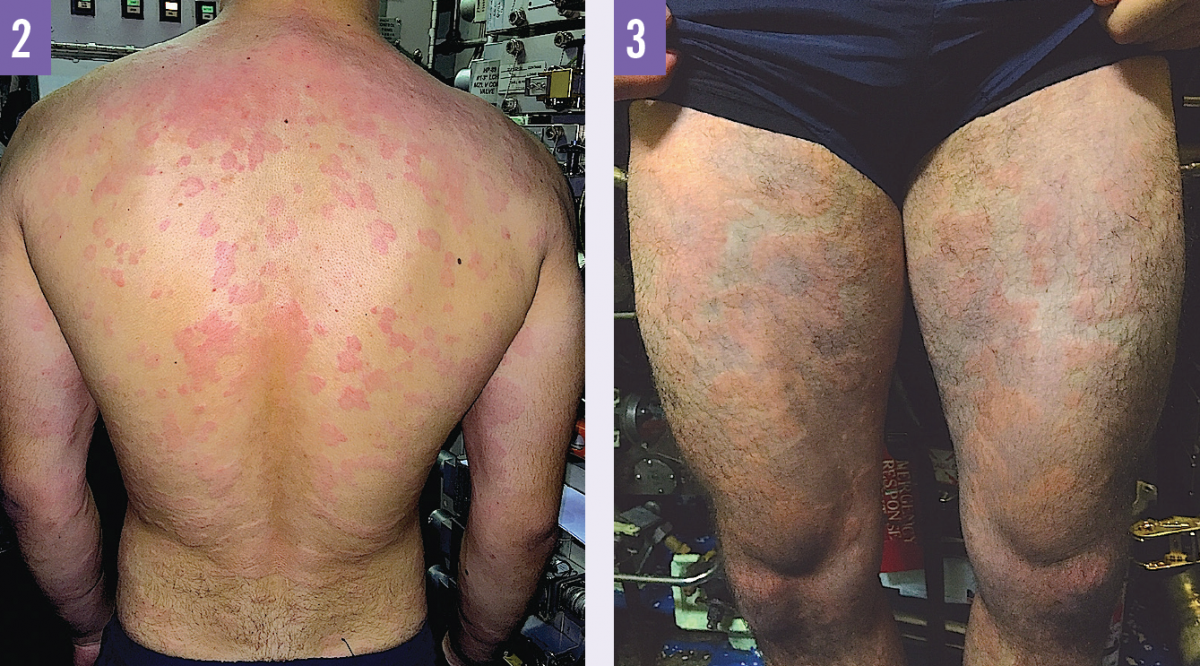
The next day, he developed a diffuse eruption on his back, chest, and thighs, in addition to the lesions still present on his arms (Figures 2 and 3), all of which were associated with intensifying pruritus.
Physical examination. On physical examination, the man’s arms, back, chest, and thighs demonstrated diffuse, erythematous, raised, circumscribed plaques and swelling; the skin was otherwise clean and intact.
Diagnosis. The patient received a clinical diagnosis of urticaria secondary to monoethanolamine (MEA) sensitivity.
Discussion. MEA is used aboard submarines in carbon dioxide (CO2) scrubbers, which serve to remove CO2 from the atmosphere. Allergic reaction secondary to MEA sensitivity is an increasingly prevalent condition being encountered in the submarine community.
Patch testing with MEA is not normally performed given the caustic nature of the substance. The diagnosis of MEA sensitivity is primarily clinical, based on symptom resolution after the strict avoidance of the compound in the atmosphere. MEA sensitivity is more prominently found in metal workers who are exposed to water-based metal working fluids.1
While second-generation antihistamines are the recommended first-line therapy for acute urticaria,2 submarines typically carry only first-generation antihistamines; as such, this patient received diphenhydramine as the initial treatment. A brief course of oral glucocorticoids can be added to antihistamine therapy to control persistent and severe symptoms.3 Antihistamines should be continued during and after the course of prednisone to minimize recurrence of symptoms, with tapering or discontinuation of glucocorticoids.
Intramuscular epinephrine should be administered in cases of anaphylaxis,4 which is distinguished from generalized urticaria by the additional involvement of respiratory compromise and/or reduced blood pressure, leading to end-organ dysfunction.5 Topical corticosteroids are the first-line treatment for allergic contact dermatitis,6 which is characterized by erythematous, indurated, scaly plaques, with vesiculation and bullae in severe cases. Allergic contact dermatitis typically is localized to the skin areas that come in contact with the allergen, with diffuse distribution occurring through secondary spread from the primary site to other areas of the body.6
Outcome of the case. Despite continuous administration of antihistamines and oral corticosteroids, the symptoms did not fully resolve until the patient boarded off the submarine 4 days later and was no longer exposed to MEA. Resolution of symptoms after avoidance of the submarine atmosphere highly suggested sensitivity to the MEA compound.
References:
- Lessmann H, Uter W, Schnuch A, Geier J. Skin sensitizing properties of the ethanolamines mono-, di-, and triethanolamine: data analysis of a multicentre surveillance network (IVDK) and review of the literature. Contact Dermatitis. 2009;60(5):243-255.
- Zuberbier T, Asero R, Bindslev-Jensen C, et al. EAACI/GA2LEN/EDF/WAO guideline: management of urticaria. Allergy. 2009;64(10):1427-1443.
- Pollack CV Jr, Romano TJ. Outpatient management of acute urticaria: the role of prednisone. Ann Emerg Med. 1995;26(5):547-551.
- Simons KJ, Simons FE. Epinephrine and its use in anaphylaxis: current issues. Curr Opin Allergy Clin Immunol. 2010;10(4):354-361.
- Sampson HA, Muñoz-Furlong A, Campbell RL, et al. Second symposium on the definition and management of anaphylaxis: summary report—Second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposium. J Allergy Clin Immunol. 2006;117(2):391-397.
- American Academy of Allergy, Asthma and Immunology; American College of Allergy, Asthma and Immunology. Contact dermatitis: a practice parameter. Ann Allergy Asthma Immunol. 2006;97(3 suppl 2):S1-S38.