
Unusual Radiographic Findings in a Girl With Crohn Disease
A 9-year-old girl, newly diagnosed with Crohn disease, had had a good clinical response with resolution of her symptoms after treatment with prednisone and mesalamine. Accordingly, the prednisone was stopped, and the mesalamine was continued to maintain remission.
After 4 months, while on mesalamine, she had an acute exacerbation of Crohn disease with abdominal pain and altered bowel habits. Prednisone was restarted, but her symptoms continued and worsened.
Kidneys, ureters, and bladder (KUB) radiograph of the abdomen (Figure 1) and computed tomography (CT) scan of the abdomen and pelvis (Figure 2) were obtained.

How do you interpret these images?
A. Intestinal polyposis
B. Pneumatosis intestinalis
C. Intraluminal gas
D. Intestinal necrosis
(Answer and discussion on next page)
Answer: B, pneumatosis intestinalis
Because the KUB radiograph (Figure 1) revealed an unusual gas pattern in the right upper quadrant, abdominopelvic CT was ordered. The coronal CT scan revealed extensive pneumatosis intestinalis (PI) involving the ascending and transverse colon (Figure 2). The scan did not show any free air in the girl’s peritoneal cavity.
Figure 1. KUB radiograph of the abdomen showed a mottled gas pattern in the right upper quadrant.
Figure 2. Coronal CT scan of the abdomen showed a curvilinear collection of gas within the bowel wall.
Prednisone was discontinued upon hospitalization, while mesalamine was continued. The patient also was started on an intravenous antibiotic regimen of ciprofloxacin and metronidazole. Her enteral feedings were stopped, and parenteral nutrition was begun. Her gastrointestinal pain and altered bowel habits began to improve.
Upon completion of 10 days of intravenous antibiotics therapy, oral feedings were initiated. This time, 6-mercaptopurine was added along with mesalamine to maintain remission. Three weeks later, a low-dose abdominal CT scan was performed (Figure 3) and revealed near complete resolution of the PI. The girl continued to do well at the 2-month follow-up visit.
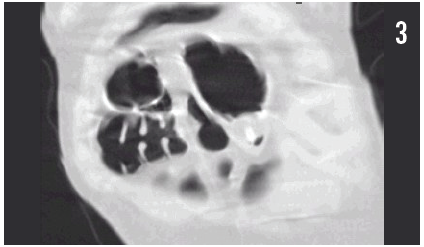
Figure 3. Three weeks after discontinuation of prednisone, coronal CT scan of the abdomen showed near complete resolution of PI.
Crohn disease (CD) is an immune mediated inflammatory disease that affects any part of the gastrointestinal tract from mouth to anus. It manifest in childhood or adolescence in up to 25% of patients. The pathophysiology is a complex interaction of various causes and current theories suggest that genetics and environment plays a significant role in dysregulation of the immune system in CD.
The most common symptoms in CD are abdominal pain, diarrhea, blood in the stool, weight loss, low-grade fever, and fatigue. Other extraintestinal symptoms such as arthritis, anemia, linear growth failure, and perianal lesions (eg, fistulae, abscesses) also are common. The primary goal of treatment is achieving and maintaining remission, thereby optimizing growth and pubertal development and avoiding disease-related complications. Remission can be achieved through the use pharmacologic agents, surgical interventions as needed, and adequate nutritional support. Various medications are used to reduce inflammation and to maintain remission; they include corticosteroids, aminosalicylates, antibiotics, immunosuppressive agents (eg, thiopurine, methotrexate), and biologic agents (eg, infliximab, adalimumab).
Short-term corticosteroid regimens traditionally have been the mainstay of treatment for inducing remission in the event of an acute flare-up of CD. Potential adverse effects of corticosteroids are cushingoid facies, changes in personality, acne, weight gain, muscle weakness, insomnia, depression, abdominal pain, osteoporosis, blurred vision, and avascular necrosis of the hip joint. PI is a rare side effect of corticosteroid use.
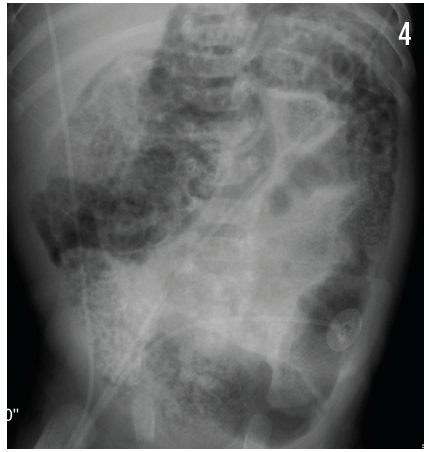
Figure 4. KUB radiograph of a different patient with a cystic, bubbly pattern of PI throughout the colon.
PI is the presence of gas within the subserosa or submucosa of the bowel wall along the mesenteric border of the intestine. Rarely, gas can be seen in muscularis propria. Two theories have been postulated about the pathogenesis of PI. The mechanical theory proposes that gas dissects into the bowel wall from either the intestinal lumen or the lung. The bacterial theory proposes that gas-forming bacilli enter the submucosa through breaks in the mucosa and produce gas within the intestinal wall.1
PI is a radiologic sign and not a disease; therefore, its significance is directly related to a patient’s overall clinical status. In the pediatric population, PI usually is seen in premature neonates with necrotizing enterocolitis; these patients are quite ill and frequently require surgical intervention. PI is an unusual finding beyond the first year of life. Late-presenting PI is associated with numerous gastrointestinal conditions such as intestinal ischemia, pyloric stenosis, bowel obstruction, blunt abdominal trauma, Hirschsprung disease, inflammatory bowel disease, and neutropenic enterocolitis,1-5 as well as pulmonary conditions such as chronic obstructive pulmonary disease, asthma, and cystic fibrosis.1,6
Medications such as immunosuppressants and α-glucosidase inhibitors can cause PI.1 The condition also has been reported in patients treated with corticosteroids following bone marrow transplantation,7 organ transplantation,8 minimal change disease,9 and various rheumatologic illnesses,1 as well as in association with certain chemotherapeutic agents.1
PI generally is diagnosed with plain abdominal radiographs. The patterns of radiolucencies appear as either linear (Figure 1) or cystic or bubbly (Figure 4), although the latter form can be difficult to distinguish from stool. CT imaging studies also can be considered.
Barium studies, ultrasonography, CT, and magnetic resonance imaging also are used. Conservative management, including bowel rest and antibiotic therapy, is the usual treatment of choice. In rare cases, development of PI-associated intestinal perforation requires surgical intervention.
In the case presented here, the patient with Crohn disease developed PI after initiation of corticosteroid therapy. Her clinical symptoms and PI resolved after discontinuation of corticosteroids. We therefore postulate that PI developed as an adverse effect of corticosteroid treatment, which initially had been used to treat an acute exacerbation of CD.
Venkedesh Raju, MD, is a pediatric hospitalist at Children’s Hospital of Illinois and a clinical assistant professor at the University of Illinois College of Medicine at Peoria.
Zahangir Khaled, MD, is a pediatric gastroenterologist at UnityPoint Health–Methodist at Peoria.
Eric Bugaieski, MD, is a pediatric radiologist at Children’s Hospital of Illinois and a clinical professor of radiology and pediatrics at the University of Illinois College of Medicine at Peoria.
Shoba Theivanayagam, MD, is a gastroenterology fellow at the University of Missouri Health Care Hospitals and Clinics in Columbia.
William Yaakob, MD—Series Editor, is a radiologist in Tallahassee, Florida.
References
1. Heng Y, Schuffler MD, Haggitt R, Rohrmann C. Pneumatosis intestinalis: a review. Am J Gastroenterol. 1995;90(10):1747-1758.
2.Gelfond D, Blanchard SS, Malkani A. Pneumatosis intestinalis: a rare presentation of Crohn disease exacerbation. J Pediatr Gastroenterol Nutr. 2011;52(2):225-226.
3. Dubinsky MC, Deslandres C, Patriquin H, Seidman EG. Pneumatosis intestinalis and colocolic intussusception complicating Crohn’s disease. J Pediatr Gastroenterol Nutr. 2000;30(1):96-98.
4. John A, Dickey K, Fenwick J, Sussman B, Beeken W. Pneumatosis intestinalis in patients with Crohn’s disease. Dig Dis Sci. 1992;37(6):813-817.
5. Matsumoto A, Isomoto H, Shikuwa S, et al. Pneumatosis intestinalis in ulcerative colitis. Med Sci Monit. 2009;15(9):CS139-CS142.
6. St Peter SD, Abbas MA, Kelly KA. The spectrum of pneumatosis intestinalis. Arch Surg. 2003;138(1):68-75.
7. Ade-Ajayi N, Veys P, Stanton M, Drake DP, Pierro A. Conservative management of pneumatosis intestinalis and pneumoperitoneum following bone-marrow transplantation. Pediatr Surg Int. 2002;18(8):692-695.
8. Fleenor JT, Hoffman TM, Bush DM, et al. Pneumatosis intestinalis after pediatric thoracic organ transplantation. Pediatrics. 2002;109(5):e78-e88.
9. Han BG, Lee JM, Yang JW, Kim MS, Choi SO. Pneumatosis intestinalis associated with immune-suppressive agents in a case of minimal change disease. Yonsei Med J. 2002;43(5):686-689.