
An Underestimated Etiology of Curable Dyspnea of the Elder: Platypnea-Orthodeoxia Syndrome
History
An 80-year-old patient was referred to our institution for hypoxemia and a disabling shortness of breath (NYHA class IV), which worsened over several weeks. The past medical history was significant only for hypertension.
Physical Examination
The exam was not very informative. The patient denied cough, fever, or chest pain. Additionally, there was no sign of heart failure. Heart sounds and chest murmur were normal. However, the patient had a tachypnea and persisting hypoxemia.
Laboratory Testing
An x-ray revealed a mild enlargement of the ascending aorta without anomaly of the lungs. A venous Doppler and a CT pulmonary artery scan did not find any venous thromboembolic diseases. Pulmonary arterial pressures assessed by transthoracic echocardiography were within normal range. There was no valvular disease. Biventricular systolic function was good. The rising aorta was slightly dilated and measured at 41 mm.
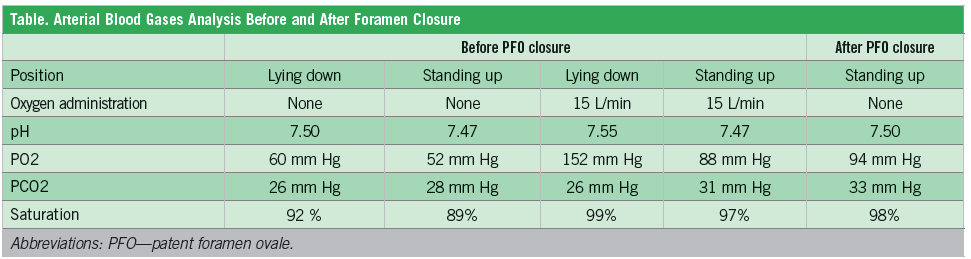
Blood gases in surrounding air revealed hypoxemia and respiratory alkalosis caused by secondary hyperventilation. This hypoxemia was not corrected by high-flow oxygen uptake, which suggests a right-to-left shunt.
Hypoxemia was observed on decubitus and increased during orthostatic trial, suggesting platypnea-orthodeoxia syndrome (POS) (Table). Diagnosis was confirmed by transesophageal echocardiography. A spontaneous right-to-left shunt through a large patent foramen ovale (PFO) was observed with color Doppler associated to an aneurysm of the interatrial septum. Contrast test confirmed a massive right-to-left shunt. No reversible trigger of the development of right-to-left shunting was found. The patient was severely affected in his daily living by this syndrome. Cognitive and physical status was not impaired after dedicated comprehensive geriatric assessment.
Treatment
After a multidisciplinary decision process, percutaneous PFO closure indication was retained. With patient informed consent, a procedure was planned under a short general anesthesia. Right heart catheterization confirmed normal pulmonary pressure.
An amplatzer PFO occluder device was inserted into the PFO to seal the passageway between the right and left atrium through a percutaneous femoral venous approach (Figure 1). IV heparin (5000 IU) and antibiotics were perfused at the beginning of the procedure.
No residual shunt was seen after placement of the PFO device on a bubble test. Oxygen peripheral saturation increased immediately. Two days later, the patient had a relief of dyspnea and was discharged at home with dual anti-platelet therapy for 3 months, followed by a mono antiplatelet therapy for an additional 3 months. During follow-up, the patient reported improvement of his functional status and of the feasibility of daily living activities.
Discussion
POS is a rare type of disabling dyspnea typically defined by the association of dyspnea and cyanosis, and exacerbated by the upright position.1 Symptoms can be less evocative and limited to fluctuating dyspnea. POS can be suspected when hypoxemia persists despite a high-flow oxygen uptake caused by a right-to-left blood shunt, typically located through a PFO.
Several anatomical factors increasing the right-to-left shunt have been identified;2 for example, an ascending aortic aneurysm may cause a distortion of the interatrial septum leading to POS.3, 4 In this patient, the eustachian valve was prominent, which lead the blood from the inferior cava vein toward the fossa ovale. A moderate dilation of a horizontal aortic root repressed atrial septum and thus, tension applied on atrial septum was lower, which caused interatrial septal aneurysm.3, 4
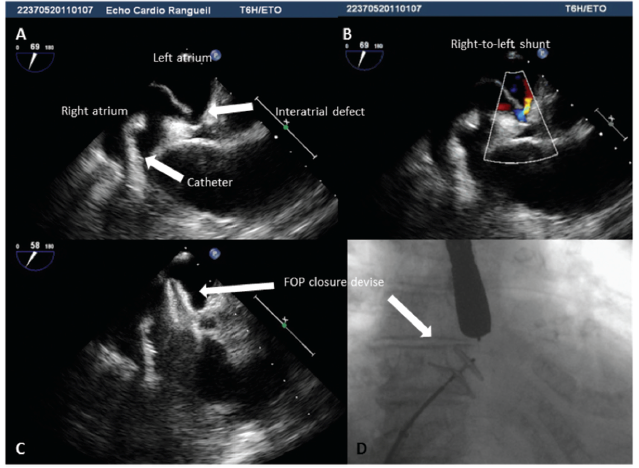
Figure 1. A: Periprocedural transesophageal echocardiography showing the large patent foramen ovale. B: Periprocedural transesophageal echocardiography with color Doppler showing spontaneous interatrial right-to-left shunt. C: Periprocedural transesophageal echocardiography showing amplatzer device positioning. D: X-ray view showing implantation procedure before device release.
Older Patients
Chronic, fluctuating dyspnea is probably one of the most challenging symptoms among elders. It is usually related to prevalent diseases, such as pulmonary embolism, pneumonia, respiratory insufficiency, or congestive heart failure. POS is a rare diagnosis that should be investigated when dyspnea mechanisms remain unclear.5 Indeed, POS usually causes disabling dyspnea, leading to a decrease in daily living activities in elders.
Paradoxical embolism and stroke are also observed in 5% to 36% of patients affected by POS. However, isolated PFO is common and observed in about 25% of the population6 without any hypoxemia-related symptoms.
Other predisposing conditions, such as pneumonectomy and kyphoscoliosis, have been described. The gradual natural history of both kyphoscoliosis and/or aortic dilation may explain the syndrome’s insidious development over years in older people.7 Reversible precipitating factors, such as pulmonary embolus, severe asthma, pneumonia,8 and right ventricular infarction may also induce an acute and transient right-to-left interatrial shunting. In these last cases, treatment of the reversible factor may cause resolution of the hypoxemia and obviate the need for PFO closure.8 Particularly, if pulmonary pressure is increased, PFO closure may precipitate right ventricular failure.
Diagnostic Tools
Blood gas (with and without oxygen) is a good screening test, usually showing insufficient rise in arterial oxygen pressure with oxygen. Contrast transthoracic echocardiography can usually detect the right-to-left shunting, but is less sensitive than transesophageal echocardiography.9, 10
Transesophageal echocardiography remains necessary to describe precisely the PFO anatomy before percutaneous closure. As shunting is usually related to inferior venous cava flowing and as shunt volume can be influenced by posture or hydratation condition, sensibility of transesophageal echocardiography can be improved by vasalva maneuvers11 or by injecting contrast through inferior venous system. Shunting may also only become apparent in the upright posture in POS.
Treatment
Over the last decade, major technical advances allow percutaneous PFO closure through venous femoral approach.12 A transjugular approach is a feasible alternative, although more challenging.13 Several devices have been developed, including the amplatzer—an auto-expandable device made of a double-disc of nitinol mesh with the memory of shape property.
Percutaneous PFO closure is usually performed under general anesthesia because of the uncomfortable transesophageal echocardiography required for procedure guidance. However, device delivering can also be performed under intracardiac echocardiography and local anesthesia. Usually, PFO closure in patients affected by POS is associated with dramatic immediate results. Indeed, shunting closure induces hypoxemia correction, rapid relief of dyspnea, and improvement in functional status.14 When PFO is not associated with POS but with cryptogenic stroke, efficiency of percutaneous closure over medical treatment remain controversial.12, 15
A large meta-analysis reported a pooled estimate rate of percutaneous PFO closure periprocedural major complications at 1.1% and minor complications at 1.3%.16 Complications are rare and mainly represented by supraventricular arrhythmia or bleeding linked with venous puncture. Severe adverse events, such as systemic thrombotic embolisms or device migration, requiring surgical intervention remain exceptional.16 Major complications during follow-up related to cerebrovascular events and device thrombosis are rare.16 These findings confirm the need for antithrombotic strategy during initial follow-up, despite a risk of bleeding particularly in older people.
Persistent right-to-left shunting through a PFO is a rare but underestimated etiology of disabling dyspnea among elders. Percutaneous PFO closure can relieve symptoms. Periprocedural and long-term complications seem rare. However, the risk-to-benefit ratio must be carefully investigated prior to PFO closure in older people.
Romain Andre, MD, is an interventional cardiologist in the CHU Toulouse, France.
Meyer Elbaz, MD, PhD, is an interventional cardiologist in the CHU Toulouse, France, specializing in coronary heart diseases and structural heart diseases.
Sebastien Hascoët, MD, is an interventional cardiologist in the CHU Toulouse, France, specializing in pediatric and adult congenital heart diseases.
References:
1. Seward JB, Hayes DL, Smith HC, et al. Platypnea-orthodeoxia: clinical profile, diagnostic workup, management, and report of seven cases. Mayo Clin Proc.1984;59(4):221-231.
2. Guerin P, Lambert V, Godart F, et al. Transcatheter closure of patent foramen ovale in patients with platypnea-orthodeoxia: results of a multicentric french registry. Cardiovasc Intervent Radiol. 2005;28(2):164-168.
3. Eicher JC, Bonniaud P, Baudouin N, et al. Hypoxaemia associated with an enlarged aortic root: a new syndrome? Heart. 2005;
91(8):1030-1035.
4. Laybourn KA, Martin ET, Cooper RA, Holman WL. Platypnea and orthodeoxia: shunting associated with an aortic aneurysm. J Thorac Cardiovasc Surg. 1997;
113(5):955-956.
5. Godart F, Rey C. Platypnea-orthodeoxia syndrome: a probably underestimated syndrome? Chest. 2001;119(5):1624-1625.
6. Fawcett E, Blachford JV. The frequency of an opening between the right and left auricles at the seat of the foetal foramen ovale. J Anat Physiol. 1900;35(1):67-70.
7. Pierce CW. Platypnea-orthodeoxia syndrome in an elderly woman with a patent foramen ovale. Can J Cardiol. 2010;26(4):
213-214.
8. Pant S, Hayes K, Deshmukh A, Rutlen DL. Hypoxemia without persistent right-to-left pressure gradient across a patent foramen ovale: a clinical challenge. World J Cardiol. 2013;5(7):254-257.
9. Cotter PE, Martin PJ, Belham M. Improved sensitivity of transthoracic contrast echocardiography in the detection of right-to-left shunts. J Am Soc Echocardiogr. 2010;23(5):578; 578-579.
10. Hegland DD, Kunz GA, Harrison JK, Wang A. Clinical problem-solving. A hole in the argument. N Engl J Med. 2005;353(22):
2385-2390.
11. Cheng TO. The proper conduct of valsalva maneuver in the detection of patent foramen ovale. J Am Coll Cardiol. 2005;45(7):
1145-1146.
12. Kwong JS, Lam YY, Yu CM. Percutaneous closure of patent foramen ovale for cryptogenic stroke: a meta-analysis of randomized controlled trials. Int J Cardiol. 2013;168(4):4132-4138.
13. Hascoet S, Fraisse A, Elbaz M. Successful percutaneous transcatheter patent foramen ovale closure through the right internal jugular vein using a steerable catheter. Catheter Cardiovasc Interv. 2013;82(4):598-602.
14. Fenster BE, Nguyen BH, Buckner JK, et al. Effectiveness of percutaneous closure of patent foramen ovale for hypoxemia. Am J Cardiol. 2013;112(8):1258-1262.
15. Rengifo-Moreno P, Palacios IF, Junpaparp P, et al. Patent foramen ovale transcatheter closure vs. medical therapy on recurrent vascular events: a systematic review and meta-analysis of randomized controlled trials. Eur Heart J. 2013;34(43):3342-3352.
16. Abaci A, Unlu S, Alsancak Y, et al. Short and long term complications of device closure of atrial septal defect and patent foramen ovale: meta-analysis of 28,142 patients from 203 studies. Catheter Cardiovasc Interv. 2013;82(7):1123-1138.