
Is there a simple diagnostic test for this treatment-resistant lesion?
Dermclinic
A Photo Quiz to Hone Dermatologic Skills
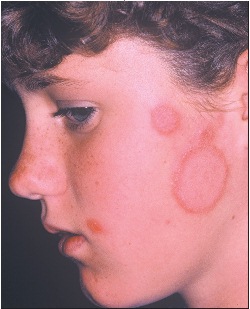
Case 1: This asymptomatic plaque on the left cheek of a 12-year-old girl was not responding to a cream that her physician had prescribed when the rash began.
Is there a simple diagnostic test? Is there an effective topical therapy?
(Answer on next page.)
 Dermclinic – Answer
Dermclinic – Answer
Case 1: Tinea faciei is a dermatophyte infection of the face that, in my experience, most often presents in childhood as misdiagnosed eczema that does not respond to topical corticosteroid therapy. As in eczema, the eruption is papulosquamous; however, the morphology and the failure to respond to topical steroids are the key elements in the diagnosis of this presentation.
The morphologic features to look for are the active inflammatory border and the tendency to central clearing that results in annular and polycyclic configurations of the plaques. The borders are not only scaly, but often papulovesicular with crusting. Also, if the follicular involvement is prominent, the lesions may look "granulomatous." The lesions appear in small numbers and are unilateral in almost all presentations.
The most useful diagnostic test is the potassium hydroxide (KOH) preparation, which can be performed as an office procedure or in your local laboratory. Take a scraping from the inside edge of the advancing border or—if a blister is present—from the underside of a blister roof.
I treat patients based on the KOH results because cultures of dermatophytes may not be available for weeks—a period during which most patients can be cured. The dermatophytes implicated in this infection are commonly zoophilic: direct skin contact with pets is the most common source of infection among affected patients in my practice. I can always imagine the gerbil, kitten, or puppy snuggling up to the cheeks of the infected child. Zoophilic dermatophytes produce the most inflammatory skin reactions but, on occasion, they will resolve spontaneously. The specific dermatophyte is often based on the regional prevalence of the dermatophytes themselves.
I attempt to treat these infections topically with an antifungal cream. More often than not, however, there is significant follicular involvement that requires systemic antifungal therapy. If 3 weeks of topical therapy with either ciclopirox or terbinafine does not eradicate the infection, I add systemic therapy with terbinafine tablets for 4 weeks.
I also recommend questioning other members of the patient’s family about scaly or itchy skin lesions that may have developed over the preceding weeks. One infected pet can affect an entire family.
Go to Case 2