
Shoe Wear Recommendations for the Older Adult
Introduction
Clinical practice suggests that many older individuals have great difficulty procuring shoes that are comfortable or shoes that successfully address a clinical problem they are experiencing. Clinicians are often faced with the difficult task of recommending shoes to their patients that will address either or both of these requirements. A report published in the Journal of the American Geriatrics Society indicated that only 58% of healthcare providers either provided intervention or made a referral for foot or footwear problems identified in their patients, with providers including Emergency Department physicians, hospital discharge planners, home health agency nurses, and primary care physicians.1 Barriers to effective intervention in these instances could include patient willingness to comply, financial resources, availability of services, and knowledge on the part of the practitioner.
The purpose of this review is to provide healthcare practitioners and the general public with information about shoe wear that might effectively address some of the common healthcare issues faced by older adults. These issues include poor balance, slipping, risk for falling, shock absorption, knee osteoarthritis, hallux rigidus, and general fit requirements. Most of the information presented in this article reflects current literature on the topics, with some suggestions arising from 30 years of clinical practice that has focused on the treatment of foot, ankle, and other lower-extremity patient problems. Summary information for each issue appears in the Table.
Poor Balance
Many shoe wear construction features have potential influence on balance, chief among these being heel lift. Menant et al2 have demonstrated that older individuals who wore shoes with a 32-mm (1.3 in) heel lift (difference between sole material underneath the heel and forefoot) had more postural sway2 and adopted a more conservative gait pattern, including increased double support time,3 as compared with a standard 14-mm (0.55 in) heel-lift shoe. Older women who wore shoes with elevated heels also demonstrated a reduction in forward functional reach and a reduced walking velocity.4 Additional support for the deleterious effects of elevated heel lift on balance comes from the work of Lord and Bashford.5 These results are probably explained by a forward shift in the center of pressure over the forefoot affected by shoes with elevated heels. Such a shift effectively reduces the ability of the shoe wearer to shift his/her center of mass safely in the forward direction. A women’s dress shoe may also result in a reduced base of support in the anterior-position/posterior direction since the distance between the forefoot and the heel of the shoe is shorter than a conventional low-heeled shoe (Figure 1a).
Clinical experience suggests that one caveat to the recommendation that older individuals wear shoes with reduced heel lift involves an older individual who has ankle joint equinus, or very limited dorsiflexion that borders on a plantar flexion contracture. Older individuals who have such pronounced tightness in the triceps surae muscle group probably will experience a posterior displacement of the center of pressure toward their heel, placing them at risk for falling backwards. One of my previous older patients received advice from a geriatric clinic that she should stop wearing her ruby-red high-heeled shoes for fear that she would fall if she continued to wear these favorite shoes. She complied with the clinicians’ wishes and proceeded to suffer several falls backwards. Assuming limited ability to elongate the tight triceps surae tissues, these patients should be encouraged to wear shoes with enough heel lift to accommodate their posterior soft-tissue tightness, without using so much heel lift that they incur the adverse consequences experienced by older subjects in the previously reviewed studies. Determination of this appropriate heel lift may require some experimentation on the part of the patient and the clinician, which may be accomplished by using pieces of heel-lift material inside the shoe, either until the patient subjectively reports feeling stable in all directions, or until the clinician can objectively document stability with clinical tests such as the Functional Reach Test4 and the Reach in Four Directions Test.6 So, heel lift should not be too high, nor too low, but just right (much like Goldilocks’ preference for porridge).
Stiffness of the sole material is another shoe construction feature that can influence balance. Menant and colleagues7 reported that use of shoes with a softer sole (Shore A-25; see Shore® test for sole hardness, described in “Slippery” section) resulted in increased postural adjustments to improve medial-lateral stability as compared with shoes with a more neutral sole hardness (Shore A-40). The detrimental effects of softer sole material on gait stability was supported by additional information from Menant et al.2,3 Shoes that have abnormally soft sole material may produce an unstable support surface, thereby adversely influencing balance in older individuals.
Additional shoe construction features that may influence balance are width of the shoe’s sole material and height of the upper material on the foot and ankle. Clinical experience suggests that older individuals have greater medial-lateral stability when the sole material of their shoes is wider. Wider sole material provides a wider base of support and ensures that the person’s center of mass is more likely to fall within that increased medial-lateral base of support. Shoes with heel lift often have a reduced width of their sole material (Figure 1b), thereby adversely affecting medial-lateral balance. Menant and colleagues3 have demonstrated in several studies that high-collar shoes, or shoes that have upper materials extending more superiorly on the foot and ankle, elicited more stable gait characteristics and greater standing stability.2 Lord et al8 also reported that these shoes elicited reduced postural sway, improved limits of balance, and had greater stability than lower-collared shoes. These shoes may have a positive influence on balance by assisting ankle musculature with anterior-posterior and medial-lateral stability around the ankle joint and proximal joints of the foot.
 In the past few years, several of my patients have asked my opinion regarding a new shoe design that has been well advertised, namely shoes with a rocker-bottom design. A popular example of this type of shoe is the MBT® (Masai Marketing & Trading AG, Switzerland), which has a convexity of the sole material such that the apex of the convexity is midway between the heel and toe of the shoe (Figure 2). This shoe design effectively creates a negative heel with less sole material underneath the individual’s heel than the thickness of sole material in the middle of the foot. Albright and Woodhull-Smith9 documented very recently that this shoe design created anterior-posterior instability during laboratory testing when a sudden anterior perturbation was imposed on their subjects. As suggested previously, use of this shoe by older individuals who have appreciably tight triceps surae would very likely produce increased risk for falling backwards. A second type of rocker-bottom design involves shoe sole material that has a relatively neutral heel structure and a rocker-bottom curvature in the forefoot region of the shoe. An example of this shoe is the Etonic Minado® (Etonic Worldwide; Westborough, MA; Figure 3). This shoe design feature will be discussed later in this article as a desirable intervention for the potentially painful condition of hallux rigidus. In response to a sudden forward perturbation of the center of mass, such as being “bumped” from behind while standing or walking, however, this shoe design also may produce anterior-posterior instability.9
In the past few years, several of my patients have asked my opinion regarding a new shoe design that has been well advertised, namely shoes with a rocker-bottom design. A popular example of this type of shoe is the MBT® (Masai Marketing & Trading AG, Switzerland), which has a convexity of the sole material such that the apex of the convexity is midway between the heel and toe of the shoe (Figure 2). This shoe design effectively creates a negative heel with less sole material underneath the individual’s heel than the thickness of sole material in the middle of the foot. Albright and Woodhull-Smith9 documented very recently that this shoe design created anterior-posterior instability during laboratory testing when a sudden anterior perturbation was imposed on their subjects. As suggested previously, use of this shoe by older individuals who have appreciably tight triceps surae would very likely produce increased risk for falling backwards. A second type of rocker-bottom design involves shoe sole material that has a relatively neutral heel structure and a rocker-bottom curvature in the forefoot region of the shoe. An example of this shoe is the Etonic Minado® (Etonic Worldwide; Westborough, MA; Figure 3). This shoe design feature will be discussed later in this article as a desirable intervention for the potentially painful condition of hallux rigidus. In response to a sudden forward perturbation of the center of mass, such as being “bumped” from behind while standing or walking, however, this shoe design also may produce anterior-posterior instability.9
In summary, shoe characteristics that can assist an older individual with balance are: avoiding shoes with elevated heel heights unless the patient has a severe ankle dorsiflexion limitation of the ankle joint; avoiding excessively soft sole material; avoiding rocker-bottom sole designs; and selecting shoes with wider sole material and a more superior collar of the upper materials. Finally, simply wearing shoes as opposed to walking in bare feet will improve balance, especially in older individuals who have impaired balance.10
Slipping
Slipping may be another concern relative to shoe wear design, since slipping may lead to a fall to the ground or injuries resulting from uncontrolled falling into objects such as chairs or tables. Sufficient friction is required to prevent unwanted slipping of the shoe on the support surface. Several investigators have provided important information regarding shoe construction features that would be protective against slipping. Tsai and Powers11 demonstrated that subjects who wore shoes with a fairly hard sole material (Shore 54D) were more likely to slip on a slippery floor surface (Teflon™) than when they wore shoes with a softer sole material (Shore 75A). The low coefficients of friction associated with harder sole materials is also supported by the work of Chaffin and colleagues.12 Sole materials of shoes are tested for hardness using the Shore® (Durometer) test.13 The Shore® (Durometer) test device measures the penetration depth of an indenter rod into the material to assess hardness, or the relative resistance to indentation. Clinicians and the general public will not have access to such a device, but they can assess the relative hardness of shoe sole material by pushing vigorously with their thumb or with a small diameter rod-like implement (eg, ballpoint pen with the pen tip retracted) into the shoe sole material to assess the relative hardness of several different pairs of shoes.
The next shoe construction feature that may have influence on an older individual slipping on a support surface may be likened to car tire technology, namely depth and width of the tread groove in the sole material. Li, Wu, and Lin14 provided original data and a nice review of pertinent literature that indicates that shoe sole material with wider and deeper tread grooves provide greater coefficients of friction and, therefore, greater resistance against slipping on floors that have liquid-contaminated conditions such as water, oil, or a detergent/water solution. The wider and deeper treads allow greater drainage of the fluid from the shoe/floor interface, thus enabling greater contact between the shoe sole material and the floor surface, and an associated greater coefficient of friction for the two-surface interface. Li and Chen15 provided additional support for the use of shoe sole materials with wider tread grooves. Both of the previously reviewed studies14,15 indicated that sole groove depth and width may be less influential in protecting against slipping when the floor surface is contaminated with oily liquids.
Older individuals who live in colder climates are often faced with the danger of slipping when walking outside on ground surfaces covered with ice. Gao et al16 have investigated this issue with particular interest since many of the older population in Sweden are injured as a result of falls on icy ground–covered surfaces. The investigators assessed type, roughness, and hardness of the sole material with regard to the coefficient of friction on ice. Only roughness was positively correlated with the coefficient of friction, suggesting that shoes with rougher (vs very smooth) sole surfaces may be protective for individuals who walk on icy surfaces.
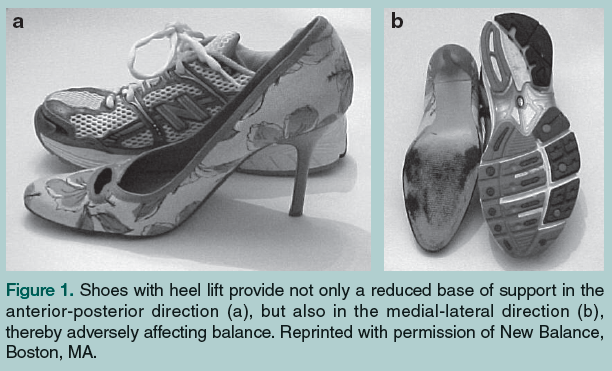
 Another strategy for prevention of slipping and falls on icy surfaces involves wearing a product such as the commercially-available Yaktrax Walker® (Yaktrax, LLC; Durham, NC). This device consists of an elastic netting that is donned over shoes or boots that will be worn on icy outdoor surfaces (Figure 4). Metal coils are wrapped around the elastic netting on the sole surface of the device. A study by McKiernan17 demonstrated that wearing this device may reduce the risk of falls outdoors during winter for older individuals. People should be warned against wearing this device on hard indoor surfaces such as tile, since the coefficient of friction between the metal coils and a hard indoor surface would be considerably low and associated with great risk for slipping. Older individuals may not want to be troubled with donning and removing this coil-like device. This author recommends that the device be applied to a pair of shoes that are dedicated for outdoor use during the winter months so that the device would not have to be removed from the shoes as often.
Another strategy for prevention of slipping and falls on icy surfaces involves wearing a product such as the commercially-available Yaktrax Walker® (Yaktrax, LLC; Durham, NC). This device consists of an elastic netting that is donned over shoes or boots that will be worn on icy outdoor surfaces (Figure 4). Metal coils are wrapped around the elastic netting on the sole surface of the device. A study by McKiernan17 demonstrated that wearing this device may reduce the risk of falls outdoors during winter for older individuals. People should be warned against wearing this device on hard indoor surfaces such as tile, since the coefficient of friction between the metal coils and a hard indoor surface would be considerably low and associated with great risk for slipping. Older individuals may not want to be troubled with donning and removing this coil-like device. This author recommends that the device be applied to a pair of shoes that are dedicated for outdoor use during the winter months so that the device would not have to be removed from the shoes as often.
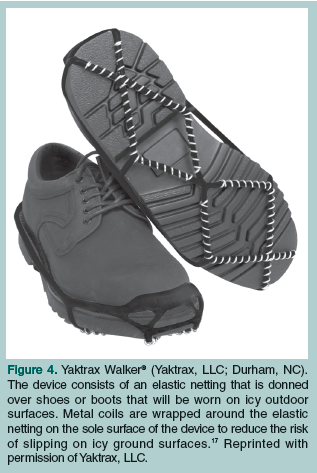
Finally, although having nothing to do with shoe construction features, a very simple intervention for prevention of slipping on any surface involves walking with a smaller step length. A reduced step length results in a lesser-magnitude anterior shearing (slipping) force imposed on the supportive surface by the shoe (Figure 5). A reduced step length also ensures that the normal component of the ground reaction force will be larger, thereby effecting a greater frictional force that will resist anterior slipping. Cooper and colleagues18 have documented that as step length increases, the required coefficient of friction to prevent slipping increases because of the previously reviewed influences of step length on the shear and normal forces.
In summary, shoe construction features that may be protective against slipping include avoiding very hard sole surfaces, wearing shoes with deeper and wider tread grooves, and wearing shoes with rougher surfaces on the sole materials.
Risk for Falling
The literature that relates shoe construction features to risk of falling is far less substantial than the previously reviewed research. The evidence for such research is much more costly in terms of time and energy, involving prospective study designs with investigators following a group of older adults over a prolonged period of time. Falls during the study period are recorded using regular contacts with the subjects, and investigators perform interviews relatively soon after each fall event to assess and record conditions at the time of the fall event, such as activity being performed, support surface conditions, and shoe wear characteristics. From this limited body of information comes the basic realization that simply wearing shoes is protective against falls. Menz et al19 prospectively followed 176 persons age 62-96 over a one-year period and found that subjects were more likely to fall indoors if they were barefoot or wearing socks as compared with wearing shoes. Wearing shoes likely increases the anterior-posterior and medial-lateral base of support, and wearing only socks probably results in a decrease in the coefficient of friction between the sock and smooth indoor surfaces such as tile flooring. Koepsell et al20 invested a phenomenal amount of resources in following 1371 adults age 65 and older over a two-year period. These investigators supported the findings of Menz and colleagues19 by detecting a sharp rise in risk for falling when their subjects were either barefoot or wearing only socks on indoor surfaces. Koepsell et al20 also reported that risk for falling was greatly reduced when subjects wore athletic-type shoes as compared with other shoe types.
Tencer and colleagues21 studied the same 1371 subject sample followed by Koepsell et al20 with regard to the biomechanical properties of the shoes worn by the subjects. Greater heel height was associated with increased risk of falling, supporting previously reviewed research that indicated increased instability with balance testing when subjects wore shoes with increased heel height.2-5 Greater surface area of the sole material, however, was associated with decreased risk of falling in subjects followed by Tencer and colleagues.21 As was reviewed in the section on balance, greater surface area that is derived from greater anterior-posterior and medial-lateral dimensions of the shoe’s sole material should ensure that the patient’s center of mass is more likely to fall within the base of support of the shoe’s sole material.
Finally, Kerse et al22 prospectively studied 606 older adults (mean age, 83 yr) living in residential care facilities. Subjects who wore slippers were at greater risk for falls as compared with subjects who wore shoes. Of the limited information available regarding risk for falls, then, older adults may reduce their risk of falling by wearing shoes and avoiding walking indoors either in bare feet or in socks alone, by wearing shoes that have lower heel heights and greater surface area of the sole material, by wearing athletic-type shoes rather than other shoe types, and by wearing shoes rather than slippers.
Shock Absorption
Clinicians often may wish to recommend shoes that will provide greater shock absorption at impact with the support surface to reduce demands for muscle-tendon force, as well as loads that are transmitted across joint surfaces. The concern for minimizing joint loads may be for the health of the articular cartilage that covers opposing joint surfaces, or for the long-term health and survival of the components for total hip and total knee replacements. Gebauer and Cziuk23 demonstrated with laboratory testing that use of a shock-absorbing shoe could be an effective and inexpensive method for long-term stability and protection of total joint components.
The ability of shoe materials to function as a shock-absorbing mechanism is based on principles of simple Newtonian mechanics given in the impulse-momentum equation:
F * Δt = m * Δv, where the ground reaction force (F) imposed on the shoe and the body acts over a period of time (Δt) to change the downward and forward velocity components (Δv) of the body’s mass (m).
The key, therefore, to minimizing the magnitude of the ground reaction force involves the deformation of shoe sole materials over the longest period of time possible, since the right side of the equation is relatively constant, assuming stable body mass and stable changes in velocity. This necessitates that the shoe sole materials have mid-range stiffness values. Sole materials that are either very stiff or that have too little stiffness will deform over a relatively shorter period of time, resulting in greater magnitude ground reaction forces. So not only heel height but also stiffness of the shoe’s sole materials can make a shoe “just right.”
For the athletic-type shoes that are protective against falls,20 shoe manufacturers attempt to achieve attenuation of ground reaction forces by incorporating air or gel cells within the sole materials to prolong the time of deformation. Alternatively, ethylene vinyl acetate (EVA) foam in the sole materials that has moderate stiffness will prolong the time of deformation, thereby minimizing the magnitude of the ground reaction forces. EVA functions as an effective shock-absorbing material through the flow of air through interconnecting cells within the material.24 The ability of EVA to function as an effective shock absorber is compromised with continued use, as the miniature air cells collapse or the thickness of the EVA is reduced. Even-Tzur and colleagues24 used finite element analyses to simulate wear of EVA materials, and they concluded that reduced thickness of the EVA material was the most important factor in repeated-use simulations that explained increased stress imposed on the human heel during ground impact. This would suggest that older individuals who would benefit from shock absorption should be counseled to select athletic-type shoes that have thicker sole materials, with moderate stiffness values (based on the “thumb or pen deformation assessment”), and should replace these shoes following prolonged use. Although not directly comparable to use for walking, Cook et al25 demonstrated that the running shoes they tested retained approximately 70% of their shock-absorbing capability after volunteers had run 500 miles in the shoes. Shoes that were initially superior in terms of their shock-absorbing capabilities had a more rapid decline in shock-absorbing capability with use as compared with shoes that were less effective shock absorbers prior to use.
An additional issue that relates to the ability of shoe sole materials to function as shock absorbers involves ambient air temperature. Dib and colleagues26 used a mechanical impact tester and assessed shoes designed with air cells, gel cells, and EVA shock-absorbing strategies. All of the shoes that were tested demonstrated significant and exponential reductions in shock-absorbing capability, as shoe temperatures decreased in 10-degree increments from +50 degrees C to -20 degrees C. The greatest decrements in shock-absorbing capability with reductions in temperature were seen at the colder end of the temperatures tested. The clinical implications for older patients who require shock-absorbing capability from their shoes is to perform weight-bearing exercise indoors rather than outside during periods of colder weather.
Knee Osteoarthritis
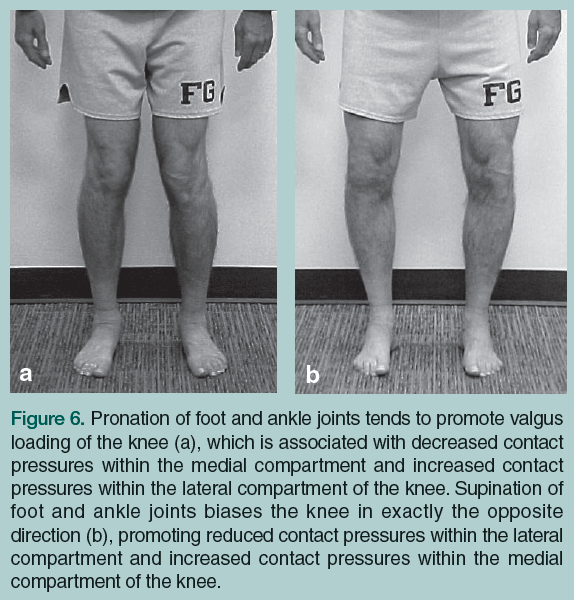
The influence of shoe wear on knee joint loads is tied to the relationship between pronation/supination of joints within the foot and ankle and frontal plane loading of the knee. Pronation of foot and ankle joints tends to promote valgus loading of the knee (Figure 6a), which is associated with decreased contact pressures within the medial compartment and increased contact pressures within the lateral compartment of the knee. Supination of foot and ankle joints biases the knee in exactly the opposite direction (Figure 6b), promoting reduced contact pressures within the lateral compartment and increased contact pressures within the medial compartment of the knee. Kemp et al27 studied frontal plane loading at the knee when subjects with medial compartment knee osteoarthrosis (OA) wore shoes as compared with walking in bare feet. Simply wearing shoes that gave some support and resistance to foot pronation will increase varus loading at the knee, thereby increasing medial compartment pressures within the knee as compared with walking in bare feet. Shakoor and colleagues28 supported this general line of logic by comparing the effects of a fairly supportive shoe (Brooks Addiction®) and a specially designed shoe that had very flexible upper and sole materials, as well as grooves cut into the sole material to promote further mobility of the shoe’s sole materials. Subjects with medial compartment knee osteoarthritis (OA) demonstrated significantly reduced varus loading at the knee when they wore the very flexible shoe as compared with the more supportive shoe.
Consistent with the previously detailed relationship between foot and knee mechanics, investigators have successfully used medially-wedged inserts to promote relative supination within the foot and reduced valgus loading at the knee for individuals with valgus malalignment and lateral compartment knee OA.29 So too, laterally-wedged insoles within the shoe have successfully driven foot pronation and reduced varus knee loading for individuals who have varus malalignment and medial compartment OA.30,31 Patients with medial compartment OA, therefore, have benefited from wearing very flexible shoes with laterally-wedged insoles.32 Conversely, patients with lateral compartment OA would benefit from medially-wedged insoles worn in very supportive shoes that would promote supination of the foot.
The final shoe construction feature that may influence knee joint loading is heel lift. Kerrigan et al33 studied older and younger women who wore standard shoes and shoes with 3.8-cm (1.5 in) heels. Both groups of women demonstrated increased varus loading and increased flexion loading at the knee during walking trials in the higher-heeled shoes. Shoes with elevated heels, therefore, would be contraindicated for patients who have medial compartment knee OA or patellofemoral joint OA. Wearing these shoes would place increased demands for quadriceps muscle contraction, thereby increasing contact pressures crossing the patellofemoral joint articulation. Elevated heels likely produce these effects, since plantar flexion is a component of supination, which promotes varus malalignment at the knee. Elevated heels also promote knee flexion, resulting in ground reaction forces being located more posterior to the knee joint center, thereby increasing knee extension moment demands from the quadriceps muscle. A study by Toda and colleagues34 supports much of the information relative to heel lift and wedged insoles by demonstrating that some of the beneficial effects of laterally-wedged insoles for decreasing varus loading in subjects with medial compartment OA were negated when they used these insoles in shoes with elevated heels.
Hallux Rigidus
Another painful condition sometimes experienced by older patients is called hallux rigidus, sometimes termed hallux limitus. This condition is characterized by pronounced hypomobility of the metatarsophalangeal (MTP) joint of the great toe, with very limited extension of the joint. Reactive bone formation on the dorsal aspect of the joint is primarily responsible for the limited motion that is seen.3 The patient is repeatedly reminded of this limitation at terminal stance when the ground reaction force produces large extension moments at the first MTP joint, attempting to force considerable MTP extension that is painful and limited.
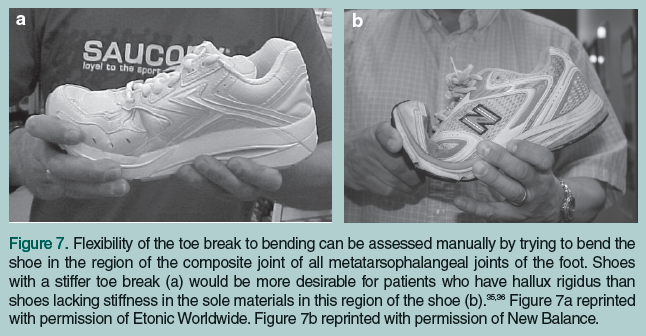
Grady et al36 retrospectively studied 772 patients with this condition and recommended intervention with a rocker-bottom sole configured similar to the one in Figure 3, combined with a shoe that has stiff sole materials. Haddad35 has made similar recommendations. Clinical experience indicates that the specific shoe  location where stiffness is desired in the sole materials is at the toe break, or the forefoot region of the shoe that bends at terminal stance. The stiffness of the toe break can be assessed manually as indicated in Figure 7a and 7b. If additional stiffness is needed to protect the first MTP joint from extension, a rigid innersole can be added inside the shoe, a rigid plate can be incorporated into the sole materials by a shoe repair shop, or a rigid plate can be added to the plantar surface of a foot orthosis (Figure 8).
location where stiffness is desired in the sole materials is at the toe break, or the forefoot region of the shoe that bends at terminal stance. The stiffness of the toe break can be assessed manually as indicated in Figure 7a and 7b. If additional stiffness is needed to protect the first MTP joint from extension, a rigid innersole can be added inside the shoe, a rigid plate can be incorporated into the sole materials by a shoe repair shop, or a rigid plate can be added to the plantar surface of a foot orthosis (Figure 8).
General Fit Recommendations and Fixation
Finally, clinicians may wish to evaluate their patients’ shoes for general fit in terms of size. My clinical experience indicates that more often than not, patients wear shoes that are too tight. Barton and colleagues37 have provided some easily implemented guidelines for the assessment of appropriateness of fit for shoes. All assessments are conducted with the patient standing in his/her shoes since the foot elongates and widens with weight bearing. Length of the shoe is assessed using the “rule of thumb.” A thumb’s width of space (10-20 mm) should be available between the end of the longest toe and the end of the shoe. Width of the shoe is assessed by grasping the upper materials across the region of the metatarsal heads to detect: excessive bunching, indicating that the shoe is too wide; slight bunching, indicating appropriate width; or whether the clinician is unable to grasp the upper materials, indicating that the shoe has insufficient width. Appropriate depth of the toe box is assessed by determining if the person can move his/her toes up and down freely and whether there is no uncomfortable pressure being imposed on the dorsal aspect of the toes and toe nails. Finally, many older adults have difficulty being able to tie shoe laces secondary to lack of strength or dexterity, or secondary to the inability to reach the shoe laces with their hands. Potential solutions to these issues are: elastic shoe laces that remain tied; long-handled shoe horns for placing the foot into the shoe; Velcro™ closures that are either placed on the shoe by the manufacturer or that can be added by a shoe repair shop following purchase of the shoes; and a long-handled grabbing device to pull the Velcro™ straps tight and secure them in place.
Conclusions
This review provides clinicians and the general public with many general recommendations for selection of shoe wear construction features that would generally be helpful in decreasing risk for slipping and falls and in improving balance and shock absorption. Additionally, recommendations for shoe wear that would be helpful for specific musculoskeletal pathologies have been made. Clinicians are encouraged to conduct thorough interviews and physical assessments with their patients prior to making any shoe wear recommendations to determine the appropriate ones for each individual.
The author reports no relevant financial relationships.
Dr. Gross is Professor, Division of Physical Therapy, Program in Human Movement Science, University of North Carolina at Chapel Hill.
References
1. Fortinsky RH, Iannuzzi-Sucich M, Baker DI, et al. Fall-risk assessment and management in clinical practice: Views from healthcare providers. J Am Geriatr Soc 2004;52:1522-1526.
2. Menant JC, Steele JR, Menz HB, et al. Effects of footwear features on balance and stepping in older people. Gerontology 2008;54(1):18-23. Published Online: February 4, 2008.
3. Menant JC, Steele JR, Menz HB, et al. Effects of walking surfaces and footwear on temporo-spatial gait parameters in young and older people. Gait Posture 2009;29(3):392-397. Published Online: January 28, 2008.
4. Arnadottir SA, Mercer VS. Effects of footwear on measurements of balance and gait in women between the ages of 65 and 93 years. Phys Ther 2000;80(1):17-27.
5. Lord SR, Bashford GM. Shoe characteristics and balance in older women. J Am Geriatr Soc 1996;44(4):429-433.
6. Newton RA. Balance screening of an inner city older adult population. Arch Phys Med Rehabil 1997;78(6):587-591.
7. Menant JC, Perry SD, Steele JR, et al. Effects of shoe characteristics on dynamic stability when walking on even and uneven surfaces in young and older people. Arch Phys Med Rehabil 2008;89:1970-1976. Published Online: August 29, 2008.
8. Lord SR, Bashford GM, Howland A, Munroe BJ. Effects of shoe collar height and sole hardness on balance in older women. J Am Geriatr Soc 1999;47(6):681-684.
9. Albright BC, Woodhull-Smith WM. Rocker bottom soles alter the postural response to backward translation during stance. Gait Posture 2009;30:45-49. Published Online: March 28, 2009.
10. Horgan NF, Crehan F, Bartlett E, et al. The effects of usual footwear on balance amongst elderly women attending a day hospital. Age Ageing 2009;38(1):62-67. Published Online: November 11, 2008.
11. Tsai YJ, Powers CM. The influence of footwear sole hardness on slip initiation in young adults. J Forensic Sci 2008;53(4):884-888.
12. Chaffin DB, Woldstad JC, Trujillo. Floor/shoe slip resistance measurement. Am Ind Hyg Assoc J 1992;53(5):283-289.
13. Shore Durometer Hardness Testing of Plastics. MatWeb Material Property Data. http://www.matweb.com/reference/shore-hardness.aspx. Accessed March 29, 2010.
14. Li KW, Wu HH, Lin YC. The effect of shoe sole tread groove depth on the friction coefficient with different tread groove widths, floors and contaminants. Appl Ergon 2006;37(6):743-748. Published Online: January 19, 2006.
15. Li KW, Chen CJ. The effect of shoe soling tread groove width on the coefficient of friction with different sole materials, floors, and contaminants. Appl Ergon 2004;35(6):499-507.
16. Gao C, Abeysekera J, Hirvonen M, Grönqvist R. Slip resistant properties of footwear on ice. Ergonomics 2004;47(6):710-716.
17. McKiernan FE. A simple gait-stabilizing device reduces outdoor falls and nonserious injurious falls in fall-prone older people during winter. J Am Geriatr Soc 2005;53(6):943-947.
18. Cooper, RC, Prebeau-Menezes LM, Butcher MT, Bertram JE. Step length and required friction in walking. Gait Posture 2008;27(4):547-551. Published Online: August 20, 2007.
19. Menz HB, Morris ME, Lord SR. Footwear characteristics and risk of indoor and outdoor falls in older people. Gerontology 2006;52(3):174-180.
20. Koepsell TD, Wolf ME, Buchner DM, et al. Footwear style and risk of falls in older adults. J Am Geriatr Soc 2004;52(9):1495-1501.
21. Tencer AF, Koepsell TD, Wolf ME, et al. Biomechanical properties of shoes and risk of falls in older adults. J Am Geriatr Soc 2004;52(11):1840-1846.
22. Kerse N, Butler M, Robinson E, Todd M. Wearing slippers, falls and injury in residential care. Aust N Z J Public Health 2004;28(2):180-187.
23. Gebauer D, Cziuk N. Analysis of the protective effect of shock-absorbing shoes for patients treated with hip and knee endoprostheses [in German]. Z Orthop Ihre Grenzgeb 1988;126(5):582-588.
24. Even-Tzur N, Weisz E, Hirsch-Falk Y, Gefen A. Role of EVA viscoelastic properties in the protective performance of a sport shoe: Computational studies. Biomed Mater Eng 2006;16(5):289-299.
25. Cook SD, Kester MA, Brunet ME, Haddad RJ Jr. Biomechanics of running shoe performance. Clin Sports Med1985;4(4):619-626.
26. Dib MY, Smith J, Bernhardt KA, et al. Effect of environmental temperature on shock absorption properties of running shoes. Clin J Sport Med 2005;15(3):172-176.
27. Kemp G, Crossley KM, Wrigley TV, et al. Reducing joint loading in medial knee osteoarthritis: Shoes and canes. Arthritis Rheum 2008;59(5):609-614.
28. Shakoor N, Lidtke RH, Sengupta M, et al. Effects of specialized footwear on joint loads in osteoarthritis of the knee. Arthritis Rheum 2008;59(9):1214-1220.
29. Rodrigues PT, Ferreira AF, Pereira RM, et al. Effectiveness of medial-wedge insole treatment for valgus knee osteoarthritis. Arthritis Rheum 2008;59(5):603-608.
30. Shimada S, Kobayashi S, Wada M, et al. Effects of disease severity on response to lateral wedged shoe insole for medial compartment knee osteoarthritis. Arch Phys Med Rehabil 2006;87(11):1436-1441.
31. Kakihana W, Akai M, Nakazawa K, et al. Effects of laterally wedged insoles on knee and subtalar joint moments. Arch Phys Med Rehabil 2005;86(7):1465-1471.
32. Fang MA, Taylor CE, Nouvong A, et al. Effects of footwear on medial compartment knee osteoarthritis. J Rehabil Res Dev 2006;43(4):427-434.
33. Kerrigan DC, Johansson JL, Bryant MG, et al. Moderate-heeled shoes and knee joint torques relevant to the development and progression of knee osteoarthritis. Arch Phys Med Rehabil 2005;86(5):871-875.
34. Toda Y, Tsukimura N. Influence of concomitant heeled footwear when wearing a lateral wedged insole for medial compartment osteoarthritis of the knee. Osteoarthritis Cartilage 2008;16(2):244-253. Published Online: August 13, 2007.
35. Haddad SL. Hallux rigidus. In: Kelikian AS, ed. Operative Treatment of the Foot and Ankle. Stanford, CT: Appleton & Lange;1999:127-146.
36. Grady JF, Axe TM, Zager EJ, Sheldon LA. A retrospective analysis of 772 patients with hallux limitus. J Am Podiatr Med Assoc 2002;92(2):102-108.
37. Barton CJ, Bonanno D, Menz HB. Development and evaluation of a tool for the assessment of footwear characteristics. J Foot Ankle Res 2009;2:10.