
Posttraumatic Stress Disorder: Psychological and Spiritual Interventions
ABSTRACT: PTSD is a trauma and stressor-related disorder that can develop after a traumatic event is experienced, and commonly involves actual or threatened death, serious injury, or threat to a person’s physical integrity, combined with feelings of intense fear, helplessness, or horror. The first article (Consultant, August 2013) introduced primary care clinicians to the history, epidemiology and diagnostic evaluation of PTSD; the second article (Consultant, September 2013) reviewed the various pharmacological treatment of PTSD. This third and final article will review the roles of therapy and spirituality.
Posttraumatic stress disorder (PTSD) is a severe condition that may develop after a person has been exposed to one or more traumatic events. Such events that may cause PTSD include violent personal assaults, natural or man-made disasters, (i.e., terrorist attacks, motor vehicle accidents, rape, physical and sexual abuse, and other crimes) or military combat. Many patients with PTSD continue to exhibit symptoms of anxiety, hypervigilance, sleep difficulties, anger, and irritability, in addition to psychological numbness and interpersonal, social, educational, and vocational dysfunctions. They also remember and often relive the traumatic events. Pharmacological interventions with various medications could relieve these symptoms.
The target symptoms of PTSD pharmacological therapy are hyperarousal, avoidance/numbing, and reexperiencing. Treatment is usually initiated with one of the serotonin reuptake inhibitors (SRIs) with a low dose that is gradually titrated to best efficacy. Reduction in PTSD symptoms usually occurs 3 to 6 weeks after the therapeutic dose of medication is reached. If the response to an SRI is inadequate, adding a second medication or switching to other antidepressants—such as mirtazapine, venlafaxine, trazodone, or sedating tricyclics (TCAs) are considered good alternatives. The sedating properties of mirtazapine and trazodone make them appropriate adjuncts to the SRIs to improve sleep disturbances and insomnia.
Primary care providers should always begin treatment protocols with low TCA doses since serum TCA levels will could increase when co-administered with the SRIs such as fluoxetine, paroxetine and to a lesser extent, sertraline and citalopram.
In difficult cases of pharmacological resistant PTSD, the monoamine oxidase inhibitor (MAOI) phenelzine can also be considered with special dietary and alcohol intake restrictions. Adjunctive therapy with prazosin is recommended in patients with nightmares. The use of atypical antipsychotics is reserved for patients with associated psychotic features or for augmenting the antidepressants effects. The mood stabilizers/anticonvulsants are not effective in the target symptoms of PTSD treatment, but are useful in treating co-occurring bipolar disorder orand in tocontrolling the associated features of anger, irritability, impulsivity, agitation, and violence.
Benzodiazepines and sedative hypnotics should be avoided, especially in patients with co-occurring alcohol and substance abuse. If a medication is well-tolerated, most patients with acute PTSD should continue to take it for 6 to 12 months. Patients who develop chronic PTSD may need to continue pharmacological treatment for at least 12 months, and as long as 24 months, before trying to taper off the medication.
If PTSD symptoms return when medication is being discontinued, the effective dose should be resumed and prescribed for a lengthier term. Patients with severe PTSD symptoms are likely to need longer treatment period. Like many chronic medical illnesses (eg, diabetes and hypertension), PTSD patients may need to be permanently maintained on medications. In some complicated PTSD cases and in patients with co-occurring medical and psychiatric conditions, the combination of various classes of psychiatric medications may be needed to accomplish a successful treatment outcome.
THERAPEUTIC TREATMENT
Psychotherapy
Unless it is contraindicated due to severe psychiatric symptoms or cognitive difficulties, psychotherapy is recommended for most PTSD patients. Psychotherapy is an effective treatment for PTSD and trauma survivors. There are a variety of psychotherapies available, but they all share common attributes of being individualized to meet the specific concerns and needs of each unique patient, based upon careful interview and questionnaire assessments at the beginning of (and during) treatment. Psychotherapy is aimed at helping patients to cope with their trauma adjust to life circumstances and to reconnect with family, friends, and society. Treatment may include individual, group, and family therapy.
Individual Therapy
•Cognitive-behavioral therapy.1,2 This type of therapy uses the principles of learning and conditioning to treat PTSD and includes components from both behavioral and cognitive therapy. In trauma-focused CBT, components such as exposure, cognitive restructuring, and various coping skills can be used either alone or in combination with one another. Most forms of trauma-focused CBT are brief and involve weekly sessions lasting 60 to 90 minutes, although the number of sessions varies across studies. CBT can be administered either as group or individual therapy.
•Prolonged exposure therapy.3,4 This therapy involves confrontation with frightening stimuli through exposure that is based on mental imagery from memory or introduced in scenes presented by the therapist (imaginal exposure). In some cases, exposure is to the actual scene or similar events in life (in vivo exposure). Exposure therapy requires PTSD patients to perform two extremely difficult tasks: intentionally confront the very memory they have been actively avoiding and trust the therapist to assist them throughout this frightening experience. This therapy is beneficial in treating combat veterans with PTSD.
•Cognitive restructuring.5,6 Based on the theory that the interpretation of the event, rather than the event itself, determines an individual’s mood, this therapy aims to facilitate relearning thoughts and beliefs generated from a traumatic event. It also helps increase awareness of dysfunctional trauma-related thoughts and correct or replace those thoughts with more adaptive and/or rational cognitions.
One example of cognitive restructuring is cognitive reprocessing, which is based on the view that fear as a cognitive structure contains representations of the feared stimuli and feared responses, as well as the meanings associated with them. In order to reduce fear, the fear memory must first be activated. Second, new information must be provided that includes elements incompatible with the erroneous elements in the existing fear structure, so that a corrected memory can be formed.
When the traumatic memories are retrieved and combined with new information, they are restored in a transformed manner with a new cognitive structure that is free from the PTSD symptoms that occurred due to traumatic cognitive distortions.
•Psychodynamic therapy.7,8 Brief psychodynamic psychotherapy focuses on intra- and interpersonal processes, not just symptom reduction, and seeks to explore unconscious and psychological meanings that have been attributed to the trauma. It uses a supportive therapeutic relationship to uncover what the specific traumatic events and circumstances mean to the individual and the obstacles to normal psychological processing of these events. It also helps patients gain insight into the relationship between the trauma and the earlier developmental experiences that may have rendered the individual vulnerable to the development of PTSD. During the therapy sessions, conflicts are reenacted and the dynamic therapists seek to help traumatized individuals re-establish a sense of coherence and meaning in their lives by identifying current life situations that exacerbate PTSD symptoms.
•Interpersonal therapy.6,9 Initially developed for the treatment of depression, the therapist facilitates the patient’s understanding of the relationships between their interpersonal behaviors and their trauma. This therapy focuses on the patient's current life events and social and interpersonal functioning to understand and treat symptoms. It may also relieve PTSD symptoms without focusing on exposure to trauma reminders. Thus, IPT may offer an alternative for patients who refuse or do not respond to exposure-based approaches.
IPT focuses on two problem areas that specifically affect patients with PTSD: interpersonal difficulties and affect dysregulation. It helps patients identify and address problematic affects, interpersonal functioning, and to monitor treatment response.
•Eye movement desensitization and reprocessing (EMDR).10,11 This therapy is based on a theory that the memory associated with traumatic or distressing events may overwhelm normal and usual cognitive coping mechanisms and as a result, the events are inadequately processed and are dysfunctionally stored in an isolated memory network. The goal of EMDR therapy is to process these distressing memories, reducing their lingering influence and allowing patients to develop more adaptive coping mechanisms.
This therapy can help change how patients react to the memories of their trauma by combining imaginal exposure with the concurrent induction of saccadic eye movements. The therapist asks the patient to contemplate memory while focusing on rapid movement of the clinicians’ fingers or other stimuli (eg, hand taps or sounds). The eye movements are believed to help reprogram brain function so that emotional impact of trauma can be resolved. In the EMDR process, the patient is instructed to imagine a traumatic memory, engage in negative cognition, and then articulate an incompatible positive cognition, such as personal worth, self-esteem, and current achievements.
•Hypnosis for posttraumatic stress disorder.1,12 People who experience trauma sometimes repress their memories of the event to avoid the pain of remembering them. These so-called repressed memories sometimes resurface during therapy or may be triggered by something in everyday experience that reminds the patient of the traumatic event. Working with repressed memories in therapy is controversial since many therapists doubt their validity and accuracy. Repressed memories are typically retrieved during hypnosis. Many psychiatrists however consider hypnosis as an unreliable tool for memory exploration and warn about the risk of worsening PTSD in patients who experienced dissociation when they were initially traumatized. However, the induction of a deep state of relaxation through hypnosis could alleviate PTSD symptoms of hypervigilance, irritability, sleeplessness, and anger in certain patients and can help them feel safer and less anxious.
•Coping skills therapy.1,13,14 This intervention includes stress inoculation therapy, assertiveness training, biofeedback, and relaxation training. The therapy uses techniques such as education, muscle relaxation training, breathing retraining, role-playing, covert modeling, thought stopping, and guided self-dialogue to manage anxiety or correct misunderstandings conditioned at the time of trauma. The therapy is designed to increase coping skills for current situations with an emphasis on problem solving.
•Mindfulness psychotherapy.1,15 Mindfulness psychotherapy is an approach aimed at reducing stress that is triggered by recalling traumatic events. The patients are taught to practice meditation with two key components: pay attention to and be aware of the present moment, and accept or be willing to experience thoughts and feelings without judgment.
 Group Therapy
Group Therapy
Groups can be process-oriented or trauma-oriented, where members tell their own story. Some focus on present-day coping skills and problem solving,6,7 while others can be psychoeducational and address specific issues, such as anger management, assertion training, substance abuse, and co-occurring disorders; other groups are specialized and use evidence-based therapy, such as CBT and IPT.18
Group therapy sessions provide mutual support from others who have experienced similar traumas and offer a forum to counter the profound sense of isolation, social withdrawal, mistrust, and loss of control. The patient’s understanding that they are not alone allows for an opportunity to support others and to build a cohesive environment where participants can safely share their traumatic experiences within a responsive and interactive personal and social context.6,7,18
Family Therapy
The inclusions of spouses, significant others, and families in treatment may be considered as an adjunct to the primary treatment of PTSD patients and it is usually time-limited and uses a problem-solving approach.6,7,18 Although patients do not spread PTSD to other family members, feelings of alienation and anger can make it difficult for other family members to communicate with the patients.18 Sleep disturbances, physical abuse, and substance use may also occur among some family members. Marital/couple therapy is typically contraindicated in cases of domestic violence, until the violent and abusing spouse has been successfully individually treated for domestic violence.6,7,18
Through a family therapy session, relatives can express their own fears and concerns. A moderator encourages others to listen, and through this interaction, the family will be better prepared to understand and help the PTSD patient.
SPIRITUALITY
Traumatic distress has been reported to be associated with spiritual alienation, which is defined as a separation from God, the transcendent, or the divine. The ability to make sense of a traumatic event in a way that “fits” with one's previous beliefs has also been reported to lead to posttraumatic spiritual growth.1,19 Patients who were able to find meaning and purpose in their traumatic experiences were less likely to develop chronic PTSD.19,20 Establishing a collaborative relationship with God, seeking divine intervention during stressful life situations, and trying to find a meaning for suffering play an integral role in thinking about one's life as a part of a larger spiritual existence.
Studies have also shown that PTSD patients with more frequent spiritual and religious practices such as prayers, worship attendance, and communing with other believers were able to regain their faith in accepting their traumatic events and turn their adversity into an opportunity for spiritual growth.18 In addition, patients with the PTSD-associated survivor guilt were able to be relieved by accepting forgiveness for their sins of commission and or omission and by forgiving those who caused the traumatic events.18,19
Primary care providers are encouraged to inquire about the spiritual component of PTSD and help their patients gain access to the meaning of their posttraumatic life. Spiritual alignment with the sense of life's purposes would lead to a structure for health, mental well-being, and healing.18-22
PTSD AND ITS PROGNOSIS
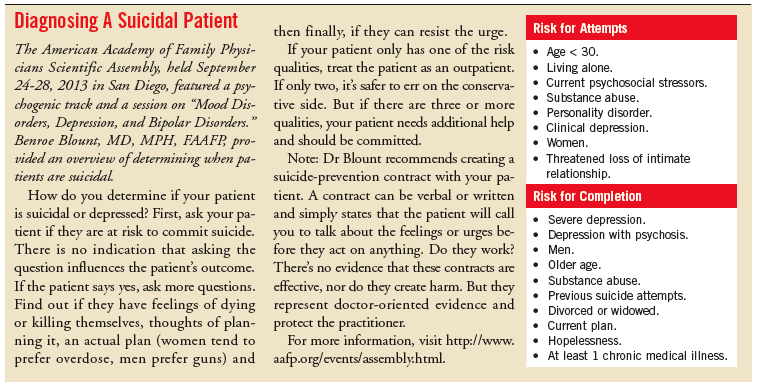
It is difficult to determine a prognosis for PTSD1,16,17 because it varies significantly from patient to patient. Some individuals who do not receive treatment gradually recover over a period of years. Many individuals who receive appropriate medical and psychiatric care are able to have a meaningful life despite the persistence of some symptoms. However, even with intensive intervention, some patients continue to experience worsening symptoms and may end their earthly existence by committing suicide. Factors associated with a good prognosis include early treatment, ongoing social support, pre-traumatic good functioning, and the absence of other co-occurring medical, psychiatric and substance abuse disorders.
Although there is no definitive cure of PTSD, it can be treated and managed through the integration of pharmacological, psychological, social, and spiritual interventions. Patients with PTSD can live a meaningful and fulfilled life with their family, friends, and community when they are encouraged and supported in adhering with acute, continuation, and maintenance treatment. Primary care provider could play a pivotal role in identifying, initially treating, and referring complicated PTSD cases to specialized care.
Acknowledgements
The author thank Ms Fionna Sutherland, team manager, and all the Cottage staff members, as well as Ms Natalie Leger, team manager, and all the Faleola Services staff members for their support, encouragement and inspiration. ■
REFERENCES
1.Conen S, Theunissen EL, Vermeeren A, Ramaekers JG. Short-term effects of morning versus evening dose of hydroxyzine 50 mg on cognition in healthy volunteers. J Clin Psychopharmacol. 2011;31(3):294-301.
2.Lynn SJ, Malakataris A, Condon L, et al. Post-traumatic stress disorder: cognitive hypnotherapy, mindfulness, and acceptance-based treatment approaches. Am J Clin Hypn. 2012;54(4):311-30.
3.Vermetten E, Lanius RA. Biological and clinical framework for posttraumatic stress disorder. Handb Clin Neurol. 2012;106:291-342.
4.Yoder M, Tuerk PW, Price M, Grubaugh AL, Strachan M, Myrick H, Acierno R. Prolonged exposure therapy for combat-related posttraumatic stress disorder: comparing outcomes for veterans of different wars. Psychol Serv. 2012;9(1):16-25.
5.Wood DP, Murphy J, McLay R, et al. Cost effectiveness of virtual reality graded exposure therapy with physiological monitoring for the treatment of combat related post traumatic stress disorder. Stud Health Technol Inform. 2009;144:223-9.
6.Böttche M, Kuwert P, Knaevelsrud C. Posttraumatic stress disorder in older adults: an overview of characteristics and treatment approaches. Int J Geriatr Psychiatry. 2012;27(3):230-9.
7.Foa EB, Keane TM, Friedman MJ, Cohen J (eds). Effective treatments for PTSD: Practice Guidelines from the International Society for Traumatic Stress Studies. 2nd ed. New York: Guilford Press; 2009.
8.Gibbons MB, Crits-Christoph P, Hearon B. The empirical status of psychodynamic therapies. Annu Rev Clin Psychol. 2008;4:93-108.
9.Rafaeli AK, Markowitz JC. Interpersonal psychotherapy (IPT) for PTSD: a case study. Am J Psychother. 2011;65(3):205-23.
10.Stramrood CA, van der Velde J, Doornbos B, et al. The patient observer: eye-movement desensitization and reprocessing for the treatment of posttraumatic stress following childbirth. Birth. 2012;39(1):70-6.
11.Nijdam MJ, Gersons BP, Reitsma JB, et al. Brief eclectic psychotherapy v. eye movement desensitisation and reprocessing therapy for post-traumatic stress disorder: randomised controlled trial. Br J Psychiatry. 2012;200(3):224-31.
12.Proescher EJ. Hypnotically facilitated exposure response prevention therapy for an OIF veteran with OCD. Am J Clin Hypn. 2010;53(1):19-26.
13. Zemishlany Z. Resilience and vulnerability in coping with stress and terrorism. Isr Med Assoc J. 2012;14(5):307-9.
14.Sones HM, Thorp SR, Raskind M. Prevention of posttraumatic stress disorder. Psychiatr Clin North Am. 2011;34(1):79-94.
15.Wahbeh H, Lu M, Oken B. Mindful awareness and non-judging in relation to posttraumatic stress disorder symptoms. Mindfulness. 2011;2(4):219-27.
16.Kingsley G. Contemporary group treatment of combat-related posttraumatic stress disorder. J Am Acad Psychoanal Dyn Psychiatry. 2007;35(1):51-69.
17.Najavits LM. Expanding the boundaries of PTSD treatment. JAMA. 2012;308(7):714-6.
18.Greenman PS, Johnson SM. United we stand: emotionally focused therapy for couples in the treatment of posttraumatic stress disorder. J Clin Psychol. 2012;68(5):561-9.
19.Löffler S, Bogausch A, Knappe R, et al. Path to growth or open wound? The quest for meaning and coping with trauma in patients with posttraumatic stress disorder. Psychosom Med Psychother. 2012;58(2):192-204.
20.Khouzam HR, Kissmeyer P. Antidepressant treatment, posttraumatic stress disorder, survivor guilt, and spiritual awakening. J Trauma Stress. 1997;10(4):691-6.
21.Schaefer FC, Blazer DG, Koenig HG. Religious and spiritual factors and the consequences of trauma: a review and model of the interrelationship. Int J Psychiatry Med. 2008;38(4):507-24.
22.Rhoades GK, McIntosh DN, Wadsworth ME, et al. Forgiving the September 11th terrorists: associations with coping, psychological distress, and religiosity. Anxiety Stress Coping. 2007;20(2):109-28.

Hani Raoul Khouzam, MD, MPH, FAPA is a consultant psychiatrist at the Matariki Community Mental Health Centre in counties Manukau, New Zealand. He is a health sciences clinical professor of psychiatry at the University of California San Francisco (UCSF) Fresno Medical Education Program and a psychiatrist at the VACCHCS in Fresnco, CA.