
Photoclinic
Foresee Your Next Patient
 Two examples of polydactyly are shown. Photos A and B show a female newborn's right hand with an almost fully developed extra thumb; the radiograph shows what appears to be the distal phalanx bone of the extra digit. The infant had no evidence of associated congenital anomalies. There was no family history of polydactyly.
Two examples of polydactyly are shown. Photos A and B show a female newborn's right hand with an almost fully developed extra thumb; the radiograph shows what appears to be the distal phalanx bone of the extra digit. The infant had no evidence of associated congenital anomalies. There was no family history of polydactyly.
Digital duplication may be radial (preaxial or thumb), ulnar (postaxial or little finger), or central. Digital duplication, a common congenital abnormality of the hand, may be bilateral; the foot may also be affected. A family history of polydactyly does not dictate the location of subsequent occurences (ie, the 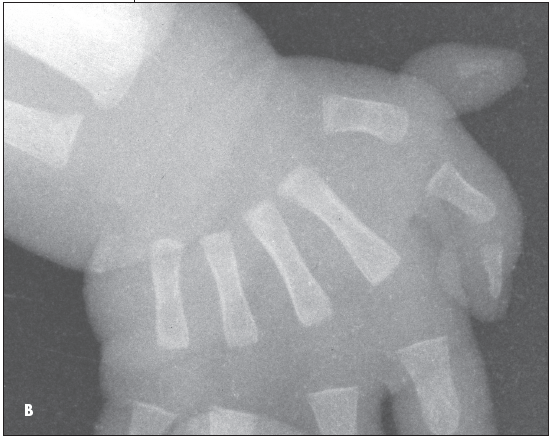 digit may not occur in the same location.) Radial polydactyly (Photos A and B) is very rare (0.08 in 1000 births). Whites are affected more than African Americans.l The male-to-female ratio is 2.5:1.1 Thumb duplication is usually sporadic. Up to 7 types have been described.2 The spectrum of duplication patterns varies from severe hypoplasia to an extrafunctional thumb.
digit may not occur in the same location.) Radial polydactyly (Photos A and B) is very rare (0.08 in 1000 births). Whites are affected more than African Americans.l The male-to-female ratio is 2.5:1.1 Thumb duplication is usually sporadic. Up to 7 types have been described.2 The spectrum of duplication patterns varies from severe hypoplasia to an extrafunctional thumb.
A postaxial extra digit usually occurs on the ulnar aspect of the fifth finger as an autosomal recessive condition in African Americans (incidence, 1 in 300).1 The condition is seldomly associated with other anomalies. In white persons, a  extra digit is 8 to 10 times less common (1 in 3000).1 However, it is more likely part of a syndrome in this group and a workup for associated anomalies thus may be warranted.3 Type B ulnar polydactyly, the most common digit duplication, usually appears as a skin tag (Photo C). (There was a history of polydactyly in this newborn's family.) In type A ulnar polydactyly, the extra little finger is more well-developed and may contain bone and other finger elements. Accessory metacarpals are not generally associated with the extra digit.
extra digit is 8 to 10 times less common (1 in 3000).1 However, it is more likely part of a syndrome in this group and a workup for associated anomalies thus may be warranted.3 Type B ulnar polydactyly, the most common digit duplication, usually appears as a skin tag (Photo C). (There was a history of polydactyly in this newborn's family.) In type A ulnar polydactyly, the extra little finger is more well-developed and may contain bone and other finger elements. Accessory metacarpals are not generally associated with the extra digit.
Type B polydactyly is treated by tying the base of the skin tag with a fine suture, which strangulates the tag. Within a few days, the tag falls off and leaves virtually no scar. Type A polydactyly and radial polydactyly require careful surgical excision usually during the end of the child's first year, when tissues are better delineated.
In patients with radial polydactyly, surgery should address both function and cosmesis. The incision, reconstruction of ligaments, and alignment of the skeleton or tendon insertions are individualized based on the pattern of duplication to preserve the best-developed thumb. ■