
 Case 1:
Case 1:
A 9-year-old girl presented with these lesions on her face and extremities. The lesions, which had developed within the past 24 hours, were warm to the touch and only mildly pruritic. The child feels unwell with nonspecific complaints of malaise and lack of energy. Before this eruption, she had been healthy and had not been taking any medications.
There is an important question to be asked in her history--do you know it?
Case 1: The diagnosis is erythema multiforme--an acute, self-limited disorder characterized by the symmetric development of papulovesicular lesions predominantly on the face and extensor aspects of the extremities. The lesions are typically only mildly pruritic, as in this patient. Involvement of the palms and soles lends great support to the diagnosis. The lesions appear in crops: a number of them develop a "target-like" morphology that, if "classic," strongly suggests this diagnosis.
Erythema multiforme (EM) primarily affects adolescents of both sexes and all races. This disorder is now considered by most of us to be different from the Stevens-Johnson syndrome/toxic epidermal 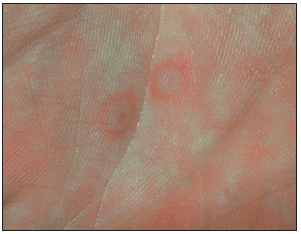 necrolysis (SJS/TEN) complex--despite some clinical and histopathologic similarities. I have discarded the concept of EM minor and major and now view SJS and TEN as severe systemic illnesses and EM as unique. The entity I describe here as EM does not evolve into SJS/TEN.
necrolysis (SJS/TEN) complex--despite some clinical and histopathologic similarities. I have discarded the concept of EM minor and major and now view SJS and TEN as severe systemic illnesses and EM as unique. The entity I describe here as EM does not evolve into SJS/TEN.
The key question is whether the child had experienced a herpes simplex virus infection within the preceding 3 to 14 days. This infection usually involves the oral labia or face, but genital herpes is also possible. Both herpes simplex 1 and 2 have been associated with EM. In over 50% of affected persons, EM is preceded by a herpes simplex virus infection--often on a recurrent basis. Herpes simplex-encoded proteins have been detected in lesions: one study found that over 80% of persons with EM had herpes simplex virus DNA in their cutaneous lesions. The argument that EM is a cutaneous reaction to herpes simplex virus infection is compelling, and although the list of putative causes of EM is long, it lends support to the theory that herpes simplex is its sole cause.
The herpes simplex lesions that precede EM may be absent or in any stage of evolution--from crust to vesicle. The typical target lesions are concentric rings of color change: the dark red center is surrounded by a ring of "clearing" and a red peripheral ring. Alternatively, the area of clearing may be absent, leaving only 2 shades of red and/or a blister in the central area. Many skin lesions are usually present in any one person; there is some grouping about the elbows, knees, and dorsa of the hands.
In addition to the possibility of oral labial lesions of herpes simplex, most children with EM have some oral involvement, however minimal. Oral erosions are usually small and well-defined: they involve the lips, buccal mucosa, and tongue.
The lesions of EM are most commonly confused with those of recurrent urticaria. The diagnosis of EM should be reserved for persons who present with fixed (in place for more than 24 hours) cutaneous lesions that all occur within 72 hours without associated edema elsewhere. If one can be specific with these criteria, the differentiation between urticaria and EM is not difficult.
Recurrent polymorphic light eruption may cause diagnostic difficulties. However, a history of sun exposure without herpes simplex lesions and the absence of the distinct cutaneous lesions of EM (target-like and oral) are useful clues. The tumid form of cutaneous lupus erythematosus may also be initially difficult to differentiate (see case 2), but the disease progression is very different.
EM is self-limited. Lesions resolve within 1 to 2 weeks without treatment. On occasion, antihistamines help with any stinging or burning of the skin. Oral corticosteroids were once thought to be useful, but studies now confirm that these agents are likely to prolong the duration and may increase the severity of EM.
The likely relationship between EM and herpes simplex virus infection has prompted the use of acyclovir in the management of EM. In my experience, however, once the cutaneous lesions of EM are present, antivirals are of little value in altering the course of the illness. Because EM often recurs following herpes simplex virus infections, I have found that prophylactic antiviral therapy has great value in preventing herpes infections. I often continue such therapy for years or reserve it for high-risk times (such as during recreational sun exposure, infections, or stress triggers) to prevent EM.
 Case 2:
Case 2:
A 14-year-old girl presents with a recurrent red swollen rash on her cheeks. She thinks that the rash tends to appear after she has been active outdoors. She is otherwise well and has no other skin lesions. She is not taking any medications.
Do you really want to biopsy this lesion (and leave a scar)? Do you have any other options?
Case 2: Cutaneous lupus erythematosus (CLE) continues to confound clinicians and test our diagnostic skills because its manifestations are protean. In my practice, lupus is the most common "great masquerader" on the skin.
I use a simple classification for CLE that first sorts the disease into acute or chronic and then subdivides it according to histology (if available):
• Acute cutaneous lupus may present as the typical malar ("butterfly") rash.
• Subacute cutaneous lupus presents with erythematous, scaling, and possibly, annular papules and plaques over the face and upper trunk.
• Tumid lupus presents as erythematous and edematous papules and plaques, as it did in this young girl.
In diagnosing CLE--particularly acute CLE--I rely heavily on the results of my clinical examination, on the patient's response to treatment, and on the disease's course over time. I look to the histopathology for assistance only if the cosmetic results of the scar from the biopsy will not be worse than the expected residual effects of the treated disease.
The histology of acute CLE often correlates with the palpability and duration of the skin lesions. The more raised the lesions are, the deeper and more cellular the infiltrate will be in the skin. Also, the longer the lesions have been present, the more developed are the changes that will be present on histologic examination. The epidermal changes mimic the cutaneous presentation (scaling, erosions, etc). The more acute lesions have the fewest histologic findings. The dermatopathologist looks for damage to keratinocytes in the epidermis and at the dermo-epidermal junction as the diagnostic feature (eosinophilic and/or liquefactive vacuolar degeneration).
I consider direct immunofluorescence (DIF) testing of the skin for acute CLE (in which the pathologist looks for a "strong" presence of granular dermo-epidermal junction deposits of IgG and/or IgM) when I am in doubt about my clinical and histopathologic diagnosis.
In tumid CLE, the histologic changes may be sparse or nonspecific. A lymphohistiocytic dermal infiltrate and mucin in the dermis are the most common findings. Results of DIF testing are often reported as nonspecific in the acute setting of tumid lupus.