
Authors:
Sameh M. Abdelaal, MBBCh, MD; Paulisa Ward, MD; and Vel Sivapalan, MD
Harlem Hospital Center, New York, New York
Citation:
Abdelaal SM, Ward P, Sivapalan V. Pseudomonas resistance in critical care units: location, location, location! Consultant. 2019;59(3):67-68.
Pseudomonas aeruginosa (PsA) is a gram-negative aerobic bacillus that is notorious for causing nosocomial infections in critically ill and immunocompromised patients. Compared with those in the general hospital wards, PsA infections in the intensive care unit (ICU) are associated with prolonged hospitalization and excessive morbidity and mortality. The ability of the bacteria to survive harsh conditions makes it easy to isolate the pathogen from a variety of sources, including respiratory equipment, catheters, antiseptics (including bleach), soaps, sinks, and physiotherapy tools. PsA has the ability to produce biofilms and survive with sparse nutrients, and it possesses an intrinsic resistance to antibiotics, making PsA infections a challenge to treat.1-6
The mechanisms of antibiotic resistance include generation of extended-spectrum β-lactamase (ESBL) enzymes; incorporation of metallo-β-lactamase genes in integrons; the ability of the porin genes to enhance their expression, interfering with drug entry; the alteration of antibiotic target sites; and the ability of PsA cells to produce effective drug efflux mechanisms.1-6
Common anti-PsA antibiotics include piperacillin/tazobactam; ticarcillin/clavulanate (penicillins plus β-lactamase inhibitors); ceftazidime and cefepime (third- and fourth-generation cephalosporins, respectively); ceftolozane/tazobactam (novel cephalosporin plus a β-lactamase inhibitor); imipenem and meropenem (carbapenems); ciprofloxacin and levofloxacin (fluoroquinolones); amikacin and gentamicin (aminoglycosides); and aztreonam (monobactam). Polymyxin B, and similarly colistin (polymyxin E) are used as a last resort due to their toxicity profiles.1-6
In 2014, Sader and colleagues6 reviewed the antimicrobial susceptibility patterns of gram-negative pathogens from ICU patients in the United States and Europe from January 2009 to December 2011. For PsA isolates in the US, there was high susceptibility to amikacin, cefepime, ceftriaxone, ciprofloxacin, gentamicin, piperacillin/tazobactam, and meropenem. In Europe, there was a similar susceptibility profile. Over time, these profiles can change, with increased resistance forcing health care providers to treat infections with multiple anti-PsA antibiotics simultaneously.
Our facility, Harlem Hospital Center (HHC), has antibiograms to guide clinicians in using antibiotics for gram-positive and gram-negative organisms. However, no ICU-specific antibiograms are available for gram-negative pathogens.
The aim of our study was to express the prevalence and pattern of antibiotic resistance in PsA isolates in the ICU setting over a 3-year period at HHC.
Methods
We conducted a retrospective chart review of patients admitted to the ICU (medical and surgical) from 2014 to 2016 at HHC to identify all PsA isolates acquired at or after 48 hours of admission to the ICU. The specimen samples were grouped according to site as tracheal, urine, sputum, bronchoalveolar lavage (BAL), and blood/fluid (pleural, peritoneal, joints)/wound. Antibiotic profiles were then compared between sites and analyzed to identify which antibiotic was best suited for a specific site of infection. The susceptibility and resistance profiles were identified using an automated identification and antibiotic susceptibility testing system (VITEK-2, bioMérieux Clinical Diagnostics) according to Clinical and Laboratory Standards Institute guidelines.
A total of 154 samples were included in this study (70 tracheal, 11 urine, 24 sputum, 20 BAL, and 29 blood/fluid/wound). For each site, the numbers of sensitive specimens (S) and resistant specimens (R) were converted into percentages, then divided as S/R to produce a ratio. A ratio greater than 1 denoted sensitivity of the sample to the antibiotic, and a ratio less than or equal to 1 denoted resistance. Antibiotics were then arranged in descending order of sensitivity for each site based on the ratio (Table).
Table. Anti-PsA Antibiotics in Descending Order of In Vitro Effectiveness Based on Specimen Site.
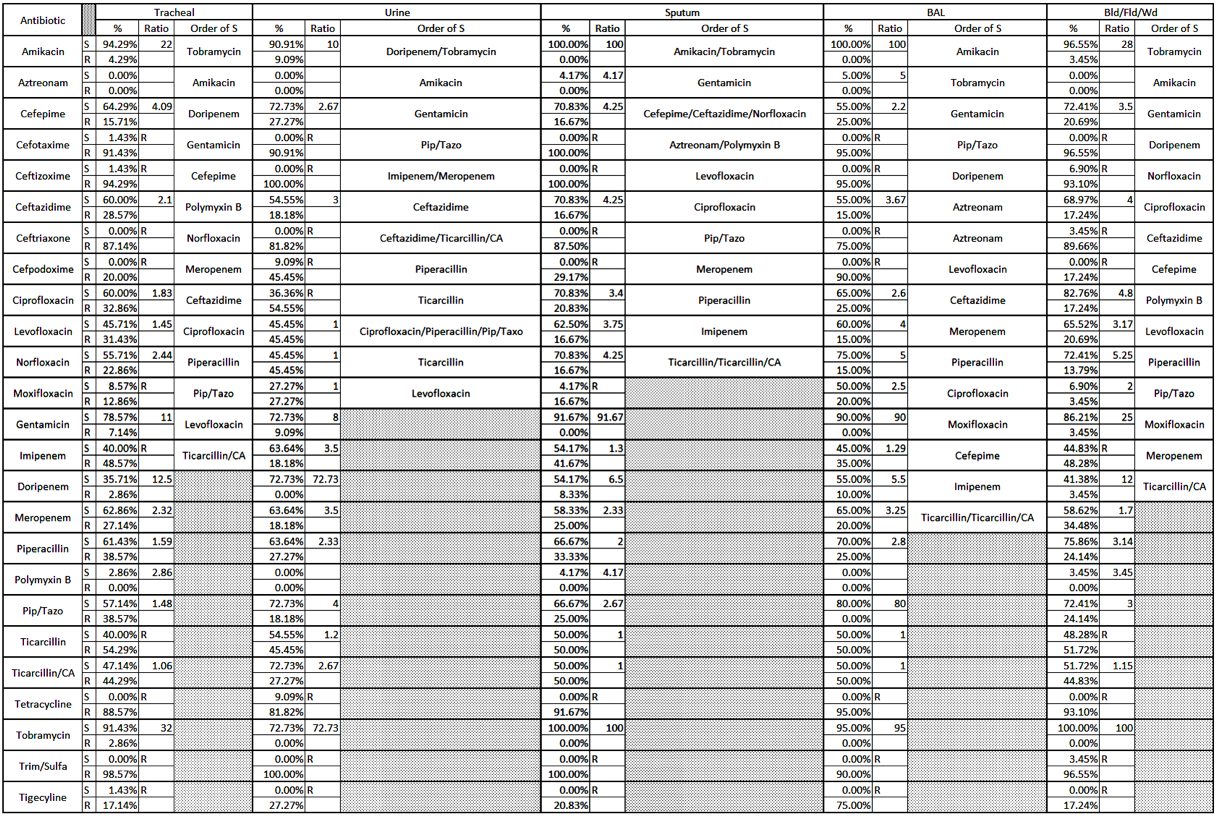
Antibiotics are arranged in an alphabetical order in the first column.
Key: S = sensitive; R = resistant; % = percentage of S and R samples; ratio = S divided by R; order of S = descending order of antibiotics from most effective to least effective.
Discussion
Tobramycin and amikacin were found to have the highest sensitivity across the specimen sources. These antibiotics are infrequently used because of their nephrotoxic and ototoxic effects. For PsA tracheal cultures, doripenem appears to be the safest alternative. BAL specimens were more sensitive to gentamicin and piperacillin/tazobactam. For urine specimens, gentamicin or ceftazidime can be used, while cefepime, ceftazidime, and norfloxacin were found to be the best suitable options for sputum. The antibiotic with the least sensitivity among all groups was ticarcillin/clavulanate, with the exception of urine, where levofloxacin was the least sensitive.
Compared with the general antibiogram for PsA in 2016, there appeared to be decreased sensitivity among most antibiotics in the ICU, a trend that is concerning for evolving bacterial drug resistance.
Nevertheless, the location of the infection may make the difference in antibiotic susceptibility. The idea can be critical with the ever-emerging resistance and is relatively a new concept for PsA that requires further research to characterize and quantize more directly. Although our study had limited power and lacks in vitro studies for newer antibiotics (eg, ceftolozane), the concept of pairing the location with susceptibility goes along the direction of more personalized—or in our study, more localized—medicine.
Conclusion
Periodic assessment of sensitivity patterns for PsA infections in the ICU is becoming increasingly important to guide antibiotic therapy and antibiotic stewardship programs, as well as to develop hospital policies regarding infection control according to site of infection. The location of infection may have a more central role for antibiotic selection than had been previously thought. As with many medical concepts, one size does not always fit all.
References:
- Izadpour F, Ranjbari N, Aramesh M-R, et al. An investigation of antibacterial resistance patterns among Acinetobacter baumannii and Pseudomonas aeruginosa isolates collected from intensive care units of a university-affiliated hospital in Ahvaz, Iran. Jundashapur J Microbiol. 2016;9(8):e35624.
- Gill JS, Arora S, Khanna SP, Kumar KH. Prevalence of multidrug-resistant, extensively drug-resistant, and pandrug-resistant Pseudomonas aeruginosa from a tertiary level intensive care unit. J Glob Infect Dis. 2016;8(4):155-159.
- Bayani M, Siadati S, Rajabnia R, Taher AA. Drug resistance of Pseudomonas aeruginosa and Enterobacter cloacae Isolated from ICU, Babol, Northern Iran. Int J Mol Cell Med. 2013;2(4):204-209.
- Işeri L, Bayraktar MR. Changes in the rates of antimicrobial resistance among clinical isolates of Pseudomonas aeruginosa between 2002 and 2004 in a tertiary-care teaching hospital in Turkey. New Microbiologica. 2008;31(3):351-355.
- de Matos ECO, de Matos HJ, Conceição ML, Rodrigues YC, Carneiro ICdRS, Lima KVB. Clinical and microbiological features of infections caused by Pseudomonas aeruginosa in patients hospitalized in intensive care units. Rev Soc Bras Med Trop. 2016;49(3):305-311.
- Sader HS, Farrell DJ, Flamm RK, Jones RN. Antimicrobial susceptibility of gram-negative organisms isolated from patients hospitalized in intensive care units in United States and European hospitals (2009–2011). Diagn Microbiol Infect Dis. 2014;78(4):443-448.