
Peer Reviewed
Syringocystadenoma Papilliferum Growth in a Nevus Sebaceous
AUTHORS:
Aspen Trautz, BS • Shaan Patel, MD, MBA • Candrice R. Heath, MD
AFFILIATION:
Lewis Katz School of Medicine, Temple University
CITATION:
Trautz A, Heath CR, Patel S. Syringocystadenoma papilliferum growth in a nevus sebaceous. Consultant. 2021;61(10):e37-e39. doi:10.25270/con.2021.01.00013
Received July 14, 2020. Accepted November 7, 2020. Published online January 29, 2021.
DISCLOSURES:
The authors report no relevant financial relationships.
CORRESPONDENCE:
Aspen Trautz, BS, MD candidate, Lewis Katz School of Medicine, Temple University, Dermatology 5th Floor Outpatient Building, 3401 N Broad Street, Philadelphia, PA 19140 (aspen.trautz@temple.edu)
A 24-year-old woman with a history of vitiligo and moderate intellectual disability had initially presented to her primary care provider for a pruritic, bleeding bump on her left parietal scalp. The papule was infected secondary to her picking, which was treated with topical antibiotics prescribed by her primary care provider. The primary care provider referred the patient to our dermatology clinic 3 months later for evaluation.
While the skin infection had resolved after treatment with mupirocin 2% ointment, the patient reported continued pruritis. Examination revealed a 0.6 cm × 0.5 cm × 0.2 cm, glistening, friable, bright red papule in the background of a scar-like pink plaque on the left parietal scalp (Figure 1). The patient was unable to provide details regarding when she first noticed the papule.

Figure 1. Gross image of the patient’s papule.
Based on characteristics of the lesion, there was initial concern for a pyogenic granuloma with chronic irritation secondary to pruritis. However, further history taken from the patient’s father at a follow-up visit revealed that a scar had been present on her scalp, in the same location as the papule, since birth. This new historical information raised suspicion for secondary development of a neoplasm in the setting of a nevus sebaceous.
The papule was shaved flat with the surrounding skin, and the specimen was sent for histopathologic evaluation. Results revealed syringocystadenoma papilliferum (Figures 2 and 3). At 6 weeks follow-up, the biopsy site was well healed with mild pruritis and no pain.
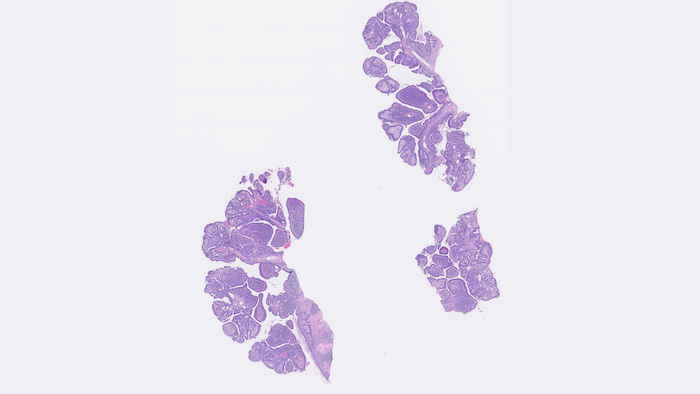
Figure 2. The low-power view shows papillary protrusions of tubular structures arising from the epidermis as well as a dense infiltrate.
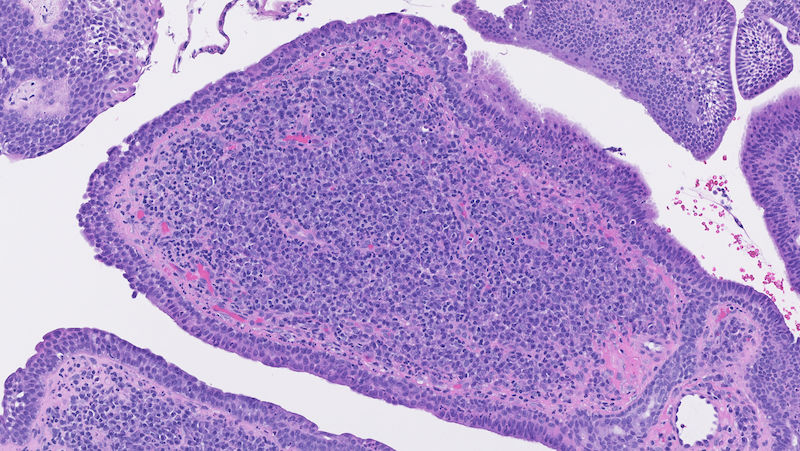
Figure 3. The high-power view shows a 2-layered epithelium with apocrine glands lining the lumen and the dermal infiltrate made of plasma cells.
Discussion. Syringocystadenoma papilliferum (SPAP) is an adnexal neoplasm that is typically present on the head or neck at birth and often enlarges at puberty. Approximately one-third of SPAPs develop within a nevus sebaceous, a benign congenital growth that is considered to be a form of an epidermal nevus.1 Various neoplasms may develop from within a nevus sebaceous, including trichoblastoma, SPAP, basal cell carcinoma, squamous cell carcinoma, and sebaceous carcinoma.
Nevus sebaceous (NS), also known as nevus sebaceous of Jadassohn (NSJ), is a hamartomatous growth most commonly present at birth that contains epidermal, sebaceous, follicular, and apocrine gland components.2 Located predominantly on the scalp and face, NSJs have been described as having 3 developmental stages based on the gross and histologic characteristics of the lesion.1,3
The initial stage spans childhood and is characterized by lobules of mature sebaceous glands with sparse eccrine and apocrine glands. Clinically, lesions appear as well-circumscribed, flat, yellow-orange plaques.1,3 When they develop on the scalp, the lesions are associated with localized alopecia. The second stage corresponds with the onset of puberty. NSJs undergo rapid growth of sebaceous glands, development of immature hair follicles, and formation of ectopic apocrine glands.1,3 Clinically, lesions tend to thicken and acquire a verrucous or nodular appearance. The final stage occurs when NSJs undergo neoplastic changes, resulting in benign and malignant tumors.1,3
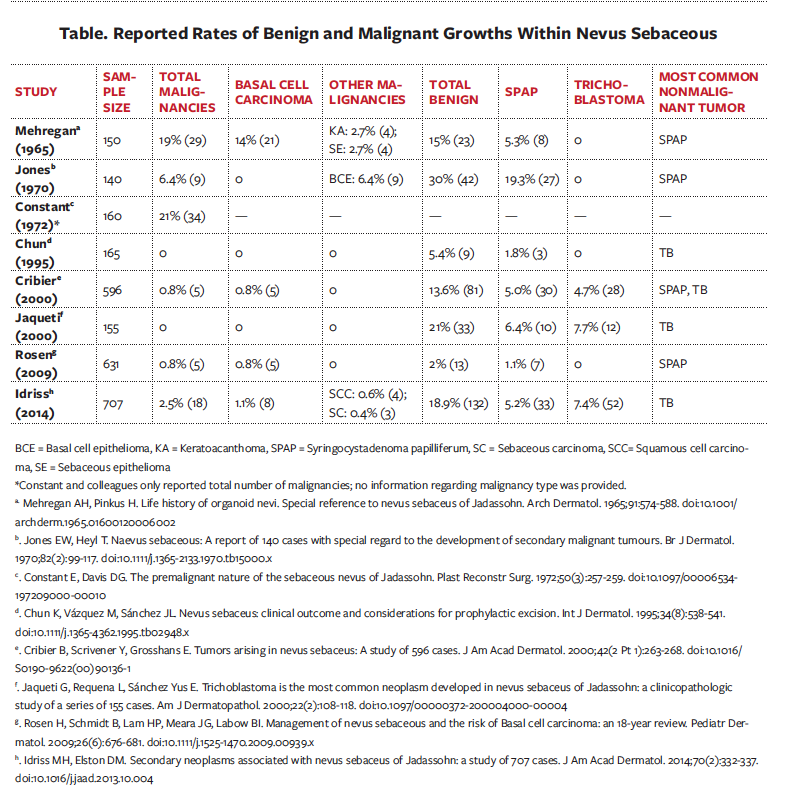
The rate of malignant transformation has been widely contested in the literature. Publications prior to 1990 tend to report 5% to 20% of tumors developing into malignancy, whereas publications from the most recent decades report much lower rates of 0% to 2.5% (Table). Bernard Cribier and colleagues4 have suggested this inconsistency is due to early publications’ misclassification of trichoblastoma as basal cell carcinoma.
Compounding the already murky etiology and progression of NSJ is recent research that suggests human papilloma virus (HPV) infection could play a role in the pathogenesis of NSJ and its secondary neoplasms.5,6 While viral warts are not among the most common secondary neoplasms seen in NS, they are present in 2.3% to 11.6% of cases.5 Previous studies6 found that HPV DNA was present in 82% of 44 NS lesions. However, these findings were not replicated in a later study,7 which found that none of their 28 samples of NS had contained HPV DNA.
Conclusion. Regardless of etiology, the rate of malignant transformation has been debated, concerning the need for and timing of NS excision. Whereas practice had previously involved proactive removal of NS lesions in early childhood, recent practice has trended toward watchful waiting with removal if cosmetically concerning or if neoplasm arises.8 As more patients are opting for the latter, it is imperative that both patients and physicians are aware of the presentations of secondary neoplasms.
References
- Alsaad KO, Obaidat NA, Ghazarian D. Skin adnexal neoplasms—part 1: an approach to tumours of the pilosebaceous unit. J Clin Pathol. 2007;60(2):129-144. doi:10.1136/jcp.2006.040337
- Jadassohn J. Bemerkugen zur Histologie der systematisirten Naevi and ueber “Talgdruesen-navi.” Arch Derm Syphilol. 1895;33:355-394. https://doi.org/10.1007/BF01842810
- Mehregan AH, Pinkus H. Life history of organoid nevi. Special reference to nevus sebaceus of Jadassohn. Arch Dermatol. 1965;91:574-588. doi:10.1001/archderm.1965.01600120006002
- Cribier B, Scrivener Y, Grosshans E. Tumors arising in nevus sebaceus: A study of 596 cases. J Am Acad Dermatol. 2000;42(2 Pt 1):263-268. doi:10.1016/S0190-9622(00)90136-1
- Richey P, Jamison M, Radfar A, DeKlotz C. New growth within a nevus sebaceous in a 10-year-old girl. J Am Acad Dermatol. 2016;74(5, Suppl 1):AB214. https://doi.org/10.1016/j.jaad.2016.02.842
- Carlson JA, Cribier B, Nuovo G, Rohwedder A. Epidermodysplasia verruciformis-associated and genital-mucosal high-risk human papillomavirus DNA are prevalent in nevus sebaceus of Jadassohn. J Am Acad Dermatol. 2008;59(2):279-294. doi:10.1016/j.jaad.2008.03.020
- Kambiz KH, Kaveh D, Maede D, et al. Human papillomavirus deoxyribonucleic acid may not be detected in non-genital benign papillomatous skin lesions by polymerase chain reaction. Indian J Dermatol. 2014;59(4):334-338. doi:10.4103/0019-5154.135475
- Patel P, Malik K, Khachemoune A. Sebaceus and Becker's nevus: overview of their presentation, pathogenesis, associations, and treatment. Am J Clin Dermatol. 2015;16(3):197-204. doi:10.1007/s40257-015-0123-y