
Peer Reviewed
A 14-Year-Old With an Inflammatory Myofibroblastic Tumor of the Bladder
Authors:
Helaine G. St. Amant, BA; Alexander Van Speybroeck, MD, MPH; and Mikako Warren, MD
Citation:
St. Amant HG, Van Speybroeck A, Warren M. A 14-year-old with an inflammatory myofibroblastic tumor of the bladder. Consultant. 2018;58(11):306-308.
A 14-year-old boy with a history of asthma and nephrolithiasis presented with a 7-day history of gross hematuria, abdominal pain, and headaches.
The hematuria had begun as bright red blood with clots and had been decreasing in volume over time but had continued to occur throughout the urinary stream with every void. He reported that the pain occurred immediately after urinating, lasted for a brief period (approximately 10 seconds) with rapid onset, and then gradually diminished. He described the pain as burning, 10 of 10 in severity, and affecting the entire groin area including the suprapubic area and the length of the penis.
Additionally, the patient reported headaches and lightheadedness that had begun approximately 3 days after the hematuria onset, requiring ibuprofen and acetaminophen as needed at home. These symptoms were associated with standing from a sitting position and playing basketball.
He denied any recent trauma, excessive exercise, or pharyngitis. He reported a recent travel history to Cabo San Lucas, Mexico, where he had consumed fruits, vegetables, ice, and seafood and had used tap water to brush his teeth.
Upon admission, the patient was afebrile, hypertensive (blood pressure, 140/78 mm Hg), and in no apparent distress. Physical examination findings were notable for sharp, 8 of 10 pain on assessment of the urethral meatus.
DIAGNOSTIC TESTS
The results of a complete blood cell count were notable for a low hemoglobin level of 8.4 g/dL and a low hematocrit value of 25.0%. Urinalysis results included a protein level greater than 300 mg/dL and were positive for 5 to 10 white blood cells per high-power field and greater than 100 red blood cells per high-power field, with positive nitrites and trace leukocyte esterase.
While evaluating the patient and interpreting preliminary laboratory test results, the differential diagnosis included possible causes for pediatric gross hematuria such as urinary tract infection, meatal/perineal irritation, urogenital trauma, nephrolithiasis, malignancy or mass, glomerular disease (eg, poststreptococcal glomerulonephritis), coagulopathies, hemorrhagic cystitis, and sickle cell disease (SCD) or trait. The patient’s medical history made coagulopathy and SCD or trait less likely, and his history of bright red blood with clots made glomerular disease less likely.
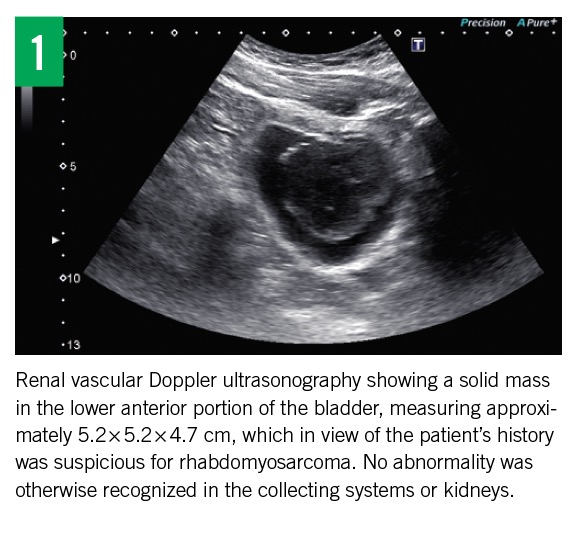
Results of abdominal computed tomography (CT) without contrast were positive for a small appendicolith and negative for nephrolithiasis. Renal vascular Doppler ultrasonography revealed a solid mass in the lower anterior portion of the bladder, measuring approximately 5.2 × 5.2 × 4.7 cm (Figure 1). These imaging findings prompted suspicion for rhabdomyosarcoma.
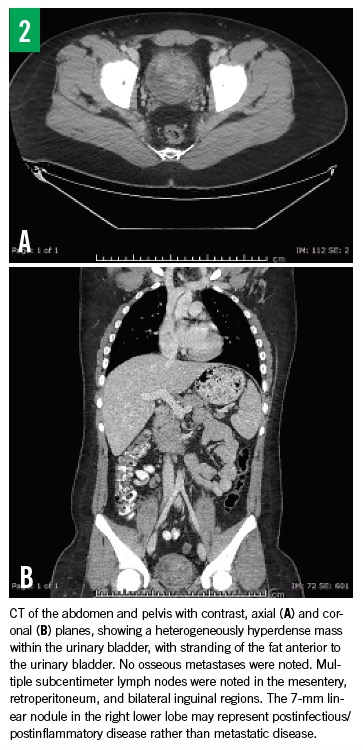
Results of repeated abdominal/pelvic CT with contrast (Figure 2) showed similar bladder findings and an additional lung nodule in the right lower lobe, which was linear and measured 7 mm—findings that were most consistent with a postinfectious or postinflammatory etiology. Nuclear medicine bone scan results did not show any lymph node enlargement or involvement.
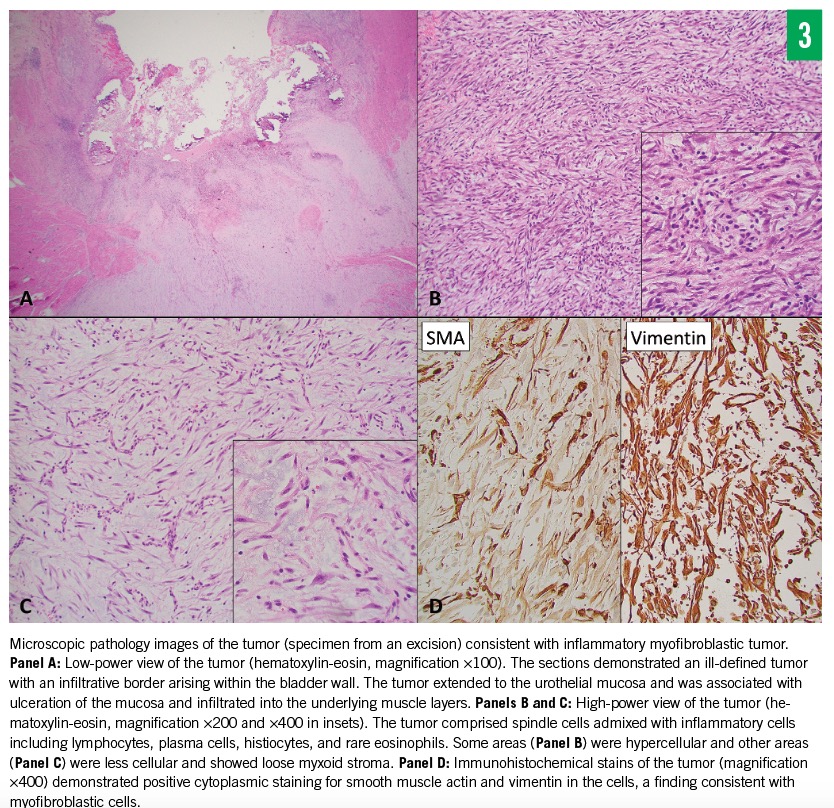
Given these findings, further diagnostic workup was indicated. Cystoscopy and transurethral biopsy were performed, and pathology results defined the mass as an inflammatory myofibroblastic tumor with anaplastic lymphoma kinase-1 (ALK-1) protein (Figure 3).
The patient underwent a transurethral resection of bladder tumor (TURBT) procedure, during which only 60% to 70% of the mass was removed due to its size. A second TURBT procedure was conducted the following day and resulted in full tumor resection with deep margins.
The patient’s postoperative course was uncomplicated. Following mass resection and Foley catheter removal, the patient required no additional pain management and urinated without any hematuria, pain, or symptoms of urinary retention. He was discharged home 24 hours after the second resection with return precautions and instructions for outpatient follow-up.
DISCUSSION
Inflammatory myofibroblastic tumors are rare spindle cell neoplasms marked by a reactive proliferation of myofibroblasts.1-4 They can occur throughout the body, with an increased occurrence rate in the lungs, soft tissues, and abdominal area.1 While their malignant potential is not fully understood, most are considered benign growths.1,4
Inflammatory myofibroblastic tumors of the urinary bladder (IMTBs) represent a unique subset of these neoplasms. Approximately 25% of IMTBs occur in children.3 In a 2015 review, 42 cases of pediatric IMTBs had been reported in the literature throughout the world. The mean age of presentation was 7.5 years, with an equal male to female distribution ratio. Hematuria was the most common presenting sign.3
IMTBs are characterized by atypical spindle cell proliferation with stellate cells and lymphocytic and plasma cell infiltration.4 Immunohistochemical staining may reveal ALK-1, vimentin, smooth muscle actin or cytokeratin positivity.4 ALK-1 is considered the most useful diagnostic immunohistochemical marker because it is expressed in 35% to 59% of IMTBs.3,4 While the clinical presentation of IMTBs in the pediatric population is often concerning for rhabdomyosarcoma and other malignant tumors, the use of myogenin (a strong immunohistochemical marker for rhabdomyosarcoma) can be used to exclude this often more-feared diagnosis.4
The long-term prognosis for IMTBs is excellent following complete transurethral resection.4 Recurrence is largely associated with incomplete surgical excision, and follow-up is recommended.1,3
Helaine G. St. Amant, BA, is a medical student at the Keck School of Medicine of the University of Southern California in Los Angeles, California.
Alexander Van Speybroeck, MD, MPH, is an attending pediatrician in the Division of General Pediatrics at Children’s Hospital Los Angeles, medical director of the Children’s Hospital Los Angeles Spina Bifida Program, and codirector Children’s Hospital Los Angeles Residency Program Global Health IMPACT Tract Program in Los Angeles, California.
Mikako Warren, MD, is a pediatric pathologist and attending physician in the Division of Pathology and Laboratory Medicine at Children’s Hospital Los Angeles in Los Angeles, California.
REFERENCES:
- Alaggio R, Cecchetto G, Bisogno G, et al. Inflammatory myofibroblastic tumors in childhood: a report from the Italian Cooperative Group studies. Cancer. 2010;116(1):216-226.
- Caporalini C, Moscardi S, Tamburini A, Pierossi N, Di Maurizio M, Buccoliero AM. Inflammatory myofibroblastic tumor of the tongue: report of a pediatric case and review of the literature. Fetal Pediatr Pathol. 2018;37(2):117-125.
- Collin M, Charles A, Barker A, Khosa J, Samnakay N. Inflammatory myofibroblastic tumour of the bladder in children: a review. J Pediatr Urol. 2015;11(5):239-245.
- Rao RN, Ranjan P, Singla N, Pandey R. Inflammatory myofibroblastic tumor of the urinary bladder diagnosed by anaplastic lymphoma kinase immunostaining. Urol Ann. 2012;4(2):115-118.