Key words: wheeze, asthma, respiratory syncytial virus, bronchiolitis, exercise- induced bronchoconstriction, allergic rhinitis, viral-induced wheeze
Wheezing, the result of airway obstruction, manifests as a whistling, puffing, or squeaking sound made by air passing through narrow tracheobronchial airways. It is one of the most common symptoms of respiratory disease in childhood. Inappropriate diagnosis and treatment of a young child's wheezing can have disastrous consequences. Unfortunately, determining the cause of wheezing in children younger than 4 years can present a clinical conundrum.
The signs and symptoms of wheezing may be confusing.1 Wheezy children often are mislabeled as having bronchitis, bronchiolitis, or pneumonia. A child's wheezing often is audible only for a brief period, which makes chest auscultation inconclusive and complicates detection and diagnosis. Objective tests can be especially difficult for children too young to perform the proper maneuver for optimal spirometry.1 A number of congenital and acquired conditions can also narrow the airways and cause wheezing, coughing, or both. Thus, a differential diagnosis becomes an important step in determining the cause of wheeze and in developing an effective management strategy.
This review discusses the challenges of ascertaining, understanding, and effectively treating the conditions that could manifest in a young child's wheezing. The focus is on therapeutic options that are available whether the cause of that wheezing is known or unknown.
Differential Diagnosis and Treatment
An accurate diagnosis of the cause of wheezing is difficult because many respiratory conditions can be the cause in young children.2 A review of a child's wheezing history as well as a family history of asthma or allergies or positive response to a given therapy may provide diagnostic clues. Therefore, it is important to take time to establish the diagnosis so as to provide adequate management of its source.
Foreign bodies and nonhereditary anatomic obstructions. In the large airways, foreign bodies can cause recurrent wheezing that, at times, may appear to be responsive to asthma controller medication. If such an obstruction is diagnosed based on a clinical examination and radiographic evidence, a bronchoscopic or surgical procedure can be performed to remove it. Any mass--such as enlarged lymph nodes or a tumor that compresses the large airway--can also cause symptoms that resemble wheezing. A chest radiograph, CT scan, or biopsy usually enables a diagnosis of such a mass. Treatment depends on its cause.
Bronchopulmonary dysplasia is the result of prematurity and intubation. The condition is diagnosed based on clinical history and physical examination and is managed with aerosolized medications and oxygen.
Hereditary and biochemical disorders. Congenital deformities in or around the large airways also can lead to wheezing. A barium esophagram or direct laryngoscopy can diagnose vascular rings or laryngeal webs; the treatment for both is surgery. Laryngotracheobronchomalacia, diagnosed by laryngoscopy or airway fluoroscopy, usually resolves spontaneously; in severe cases, however, tracheostomy may be required.
Diseases that affect the small airways, such as cystic fibrosis, also can be the source of wheezing in young children. Cystic fibrosis--a hereditary recessive disease that affects multiple organs, including the lungs--results from a defect in chloride ion transport. A clinical examination and an analysis of sweat electrolytes (chloride level exceeds 60 mmol/L in affected patients) form the basis of a cystic fibrosis diagnosis. Children with cystic fibrosis have a history of fever, failure to thrive, diarrhea, sinusitis, and recurrent pneumonia confirmed by chest radiographs. They usually are treated with aerosolized drugs, chest physical therapy, and enzyme replacement.
Immunodeficiency. Infants who have deficiencies in IgA and IgG experience frequent episodes of sinusitis, otitis media, and pneumonia; these sometimes are associated with bronchospasm and wheezing. To diagnose such a disorder, a complete blood cell count with differential and quantitative immunoglobulins should be performed. Therapy involves aggressive treatment of the infections and, possibly, intravenous immunoglobulin.
Other causes. Other causes of wheezing include GERD and tracheoesophageal fistula. GERD can be diagnosed by pH probe or endoscopy. A barium esophagram and fluoroscopy establish the diagnosis of tracheoesophageal fistula, which can be corrected surgically.
Some of the above conditions can be quickly ruled out based on the clinical presentation alone, but others may require one or more procedures or tests. Once all these possible causes of wheeze are eliminated, consider the diagnosis of asthma and implement appropriate treatment for that condition.
 Table 1 summarizes the differential diagnosis of wheezing and the therapeutic approach for each condition.
Table 1 summarizes the differential diagnosis of wheezing and the therapeutic approach for each condition.Infant wheezing--persistent or transient. Up to 50% of preschool children experience at least 1 episode of wheezing. In about two thirds of these children, episodes are transient (the child is no longer wheezing at age 6 years); in about one third, the episodes persist (the child is still wheezing at age 6 years). Transient wheezing is common and not associated with asthma later in life; however, it is associated with viral infections, smaller airways, lung size, male gender, low birth weight, and maternal smoking,3 as well as lower levels of lung function (VmaxFRC). In contrast, persistent wheezing is associated with asthma later in life3 and with maternal asthma, maternal smoking, rhinitis apart from colds, eczema during the first year of life, and male gender. Persistent wheezing is also associated with Hispanic background and reduced lung function by age 6 years.4
Viral-associated wheeze. Wheezing develops in response to a viral infection in many infants with and without asthma. The most significant wheeze-associated viruses are respiratory syncytial virus (RSV), parainfluenza, and rhinovirus. RSV is the main viral cause of wheezing in children younger than 2 years but recently, rhinovirus has been implicated as well.5
RSV is the most common infectious cause of bronchiolitis and wheezing among infants. In an infant with RSV infection, the first signs may be profuse rhinorrhea and pharyngitis, followed by coughing, wheezing, sneezing, and a low-grade fever. The diagnosis can be made by history and physical examination and by demonstrating the presence of RSV antigen in nasal secretions. The symptoms of bronchiolitis most likely result from airway inflammation. Furthermore, RSV infection is a strong independent risk factor for subsequent airway disease, such as asthma.6
Therapeutic options for viral-induced wheeze are limited. Antiviral therapy in the treatment of acute bronchiolitis has been controversial. Although early ribavirin treatment reduced the incidence and severity of airway disease and related hospitalization,7 a 1-year follow-up in infants with moderately severe acute bronchiolitis failed to demonstrate any clinical benefit.8
The pediatric guidelines1 recommend initiating therapy with a short-acting bronchodilator, although only modest short-term improvements have been observed. If wheezing episodes occur frequently, controller therapy such as inhaled corticosteroids (ICS)--with or without oral steroids--should be used.1 These agents may bring some benefit, but clinical trials have provided lit- tle evidence to support their use for wheeze-associated bronchiolitis caused by RSV. Studies in infants have shown no benefit from nebulized budesonide for either symptoms of acute bronchiolitis or the prevention of post-bronchiolitic wheezing.9 Furthermore, oral prednisolone did not prevent post-bronchiolitis wheeze or asthma in children with acute-phase RSV bronchiolitis.10
An increase in inflammatory mediators in nasal lavage fluids, especially the leukotriene C4 levels, has been shown with RSV bronchiolitis11 and after infection with rhinovirus or influenza A virus.12 Consequently, the leukotriene receptor antagonists (LTRAs) may have a potential role in bronchiolitis therapy. Infants with acute RSV bronchiolitis, aged 3 months to 36 months, who received montelukast (5 mg) were symptom-free on 22% of 28 days and nights, compared with only 4% of the infants given placebo.13 An impact of montelukast on viral-induced wheeze was supported by the Prevention of Viral-Induced Asthma (PREVIA) study.14 These results suggest that an LTRA could be used as an effective therapy for viral-induced wheeze, particularly for RSV but possibly for other viruses as well.
Exercise-induced bronchoconstriction-associated wheeze. Vigorous and unpredictable exercise and laughter, which are common behaviors for all children, can cause significant episodes of airflow obstruction and subsequent wheeze that can be difficult to manage. Although the mechanism of exercise-induced bronchoconstriction is not fully understood, a role for inflammatory mediators has been established.
Bronchodilators (long- and short- acting ß-agonists) are often administered, but the protection can be limited in duration (3 to 12 hours). Also, tolerance may develop if these agents are used regularly for a long period.15 To treat the underlying inflammation, options include corticosteroids, cromolyn, and LTRAs. Low-dose budesonide significantly reduced the maximum fall in forced expiratory volume in 1 second.16 Similarly, inhaled cromolyn or nedocromil significantly protected against exercise-induced bronchoconstriction; however, the protective effect lasted less than 2 hours.17
Pre-exercise treatment with LTRAs has reduced exercise-induced bronchoconstriction and shortened recovery time after exercise.18 The LTRAs produce acute bronchodilation in airway smooth muscle tone within 2 hours of administration and inhibit exercise-induced bronchoconstriction. Tolerance to LTRAs did not develop for periods up to 12 weeks.19 When the response to exercise was measured 20 to 24 hours post-dosing, montelukast showed superior benefits to salmeterol (8 to 12 hours post-dosing).19,20 Furthermore, a once-daily oral LTRA regimen, with montelukast for example, takes into account children's spontaneous and unpredictable strenuous exercise.
Allergic rhinitis-associated wheeze. Allergic rhinitis (AR) can begin at any age, but the peak incidence occurs in childhood and adolescence. AR is an inflammatory disease of the nasal mucosa that initiates the release of inflammatory mediators from antigen-sensitized immune cells. Postnasal drip triggers episodes of coughing and wheezing, which suggests that the propagation of airway inflammation may occur from the microaspiration of inflammatory mediators into the lower airway.
Asthma often coexists with AR, and AR often precedes the development of asthma. Therefore, AR may be an important exacerbating factor in the development of wheezy symptoms. The association between AR and the signs and symptoms of asthma, including wheeze, has been known for years, and clinical trials have shown the importance of appropriately treating the inflammation underlying AR to improve these symptoms. For example, children with asthma and allergy symptoms were treated strictly for AR with intranasal cromolyn or intranasal beclomethasone. After 6 months, AR had improved in 95% of the children and asthma severity diminished in 84%.21 It is often difficult to distinguish between primary asthma with AR symptoms and primary AR with asthma symptoms. It is good practice to treat a patient who presents with symptoms of both diseases with therapies indicated for each.
Antihistamines are the oldest and perhaps most commonly used agents for AR. Although they effectively reduce several of the primary symptoms of AR, they are less effective for nasal obstruction.22 Patients with asthma have obtained limited benefit from antihistamines, because these agents do not completely address the underlying inflammatory process.
The newest findings in AR relate to the cysteinyl leukotrienes (CysLTs) as mediators of airway inflammation.After nasal allergen challenge in sensitive patients, CysLT levels increased in nasal fluid.After a nasal CysLT challenge, nasal airway obstruction and blood flow increased. The CysLTs are key mediators in upper airway obstruction; consequently, LTRAs can play a beneficial role in AR treatment. Zafirlukast significantly diminished nasal congestion, sneezing, and rhinorrhea.23 Montelukast significantly improved daily symptoms and quality of life; it decreased inflammation by significantly reducing the number of peripheral blood eosinophils by 16% to 17% compared with a 0% to 1% change with placebo.24,25 Thus, the LTRAs target a novel mediator of inflammation in treating AR.
If drug treatment fails, immunotherapy may be considered for AR. In general, it is effective in children but is used infrequently in very young children. Immunotherapy can diminish symptom severity and decrease the need for anti-allergy medications; however, it can be long and costly, and it carries a small risk. A new strategy is to use nonspecific immunotherapy--a recombinant human monoclonal antibody against IgE (omalizumab) to prevent the initial trigger of the allergic reaction. Omalizumab reduced serum IgE levels triggered by allergen as well as symptoms in adults with AR.26 It also reduced asthma exacerbations in children 6 to 12 years old with moderate to severe allergic asthma.27
Asthma-associated wheeze. Because bronchial asthma can lead to serious chronic illness and even death, the young wheezy child, as a potential asthmatic, must be managed carefully. Although children with severe asthma are at greater risk, the risk associated with mild asthma is significant: of those who died of asthma, approximately one third had mild asthma.
The association between wheeze and asthma is intricate and complex. Wheeze does not always signify asthma, and asthma may be present without wheeze. The formidable task of identifying symptomatic infants and young children in whom asthma will develop is crucial.
 Two clinical indices have been developed to define the risks that asthma will develop in young children with recurrent wheeze: a stringent index and a loose index (Table 2).28 Asthma was 4.3 to 9.8 times more likely to develop in children 6 to 13 years old who had a positive stringent index than in those who had a negative index. Asthma was 2.6 to 5.5 times more likely to develop in children with a loose index.28 Of importance, a negative index was associated with a 95% chance that there would be no asthma by age 6 years.
Two clinical indices have been developed to define the risks that asthma will develop in young children with recurrent wheeze: a stringent index and a loose index (Table 2).28 Asthma was 4.3 to 9.8 times more likely to develop in children 6 to 13 years old who had a positive stringent index than in those who had a negative index. Asthma was 2.6 to 5.5 times more likely to develop in children with a loose index.28 Of importance, a negative index was associated with a 95% chance that there would be no asthma by age 6 years.Consequently, the National Asthma Education and Prevention Program (NAEPP) guidelines recommend that "the initiation of long-term therapy should be considered in infants and young children who have had more than 3 episodes of wheezing in the past year that lasted more than 1 day and affected sleep and who have risk factors for the development of asthma."1
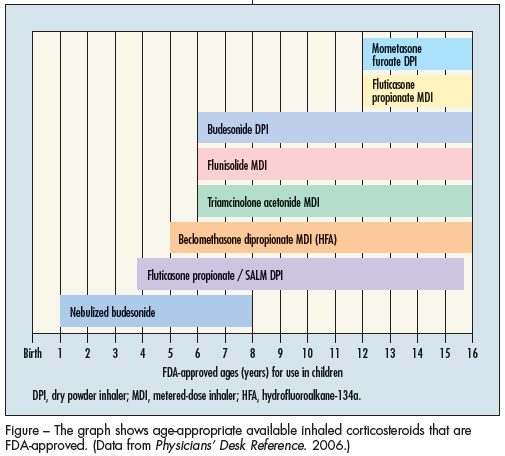
Early, aggressive, long-term ICS therapies are currently the mainstay of treatment in children with persistent asthma at any level of severity. Budesonide improved asthma symptom scores and provided greater improvement than cromolyn.29 ICS therapy improves asthma control significantly and reduces severe exacerbations and daytime and nighttime symptoms of cough, wheeze, and dyspnea; these agents also improve lung function and airway hyper-responsiveness in wheezy children. Although most ICS are approved for children aged 6 years and older (Figure),concern has been raised about their potential adverse effects--especially the risk of growth limitation.30 The changes in growth rates appear to be temporary and not predictive of adult height, however.
A recent trial documented symptom control in preschool children at high risk for asthma who were treated for 2 years with inhaled fluticasone via aerochamber with facemask.31 However, strong evidence that early treatment with inhaled corticosteroids does not modify the long-term natural history of asthma now exists from this and other trials.31-33 As would be expected, treatment with inhaled fluticasone in 1 of these trials had a negative impact on growth.31
The latest approved class of anti-asthma drugs, the LTRAs, are effective as monotherapy (for mild persistent asthma) or as an add-on to ICS therapy (for persistent asthma, any severity level) and are approved for use by children as young as 1 year.34-37 Zafirlukast improved most efficacy outcomes significantly in children with mild to moderate asthma36 and reduced the use of rescue medications.
In asthmatic children as young as 2 years, montelukast significantly improved clinical outcomes, including improved pulmonary function in older children, reduced asthma symptoms, increased activity tolerance, and improved quality of life. It also reduced b-agonist use and asthma exacerbations relative to placebo. Montelukast also significantly reduced peripheral blood eosinophils.34,35 Clinical benefits were evident within 1 day of initiation of therapy. Montelukast showed a consistent effect, regardless of concomitant ICS or cromolyn therapy. The adverse effects of either LTRA were similar to those of placebo. These results support the effectiveness and tolerability of the LTRAs for the prophylaxis and chronic treatment of mild to moderate asthma in children.
Approaches to Therapy For Wheeze of Unknown Cause
The consequences of a child's first episode of wheezing can be severe. The clinician's primary goal is to navigate the child safely through the first episode of wheezing and then consider the causes of the wheeze and evaluate the need for further therapy. Because there are no objective tests to assess the gravity of airway obstruction underlyingthe wheeze, the clinician must rely on experience and information gleaned from empiric clinical trials when treating young children. Initially, children should be examined with each wheezing episode so that a clinician can determine whether the presentation is consistent with asthma (reversible obstruction) or another disease.
Often it is necessary to distinguish between upper and lower obstructive airway diseases. The clinician may choose to treat a first wheezing episode as if it will not recur, thus not initiating a controller medication and using a bronchodilator, a steroid burst, or even nothing at all. Albuterol may be continued if the child responds to it. The child who does not respond can be considered unresponsive to bronchodilators, and the medication should be stopped. Some physicians add systemic corticosteroids, while others may stop therapy and wait for possible recurrent episodes.
The route of drug administration is critical. Difficulty in delivering medication into the airways of very young children is an obstacle to treating the wheeze adequately. Although albuterol is highly effective when successfully delivered directly into the lung, its efficacy is questionable when given orally (as a syrup). Therefore, nebulized albuterol is the first choice for wheeze in young children in the hospital, where the clinician can listen to the patient's chest before, during, and after treatment and make assessments. This offers a better opportunity for follow-up, which is important in assessing the benefits of treatment and to determine the course of further therapy.
A more aggressive approach to therapy is warranted with the sicker child or the child who is not responsive to albuterol. The clinical indices of defined risk of asthma28mentioned above may have important implications in determining the course of therapy, especially for children at high risk.
Ultimately, the use of any index of risk must consider the benefit-to-risk ratio of the recommended therapy. For example, a treatment with high efficacy and potentially significant adverse effects could be used only in children with a high risk of disease. On the other hand, lower efficacy therapy with few or no adverse effects could be sufficient for children with a positive loose index.
ConclusionsSevere disability and even death can result from the inappropriate diagnosis and treatment of a young child's wheezing. However, identifying the causes of wheeze, which are not all exclusive of one another, presents a significant clinical challenge. Viral respiratory infections, exercise, AR, or asthma can be a source of the wheeze.
The treatment of wheeze requires follow-up of the initial episode to determine treatment outcome and recurrence and a balance of safety and efficacy.38With the difficulty of diagnosing the specific cause of wheeze in young children, there is a risk of misdiagnosing it. If the risk of therapy is less than the risk of the disease (eg, asthma), the treatment can be initiated and subsequently discontinued if it is determined that the child does not have asthma.